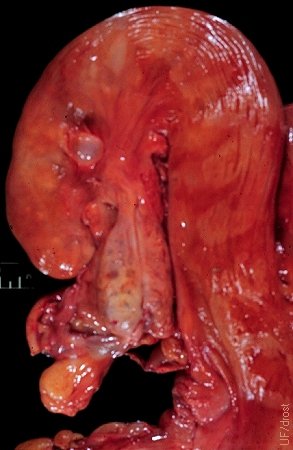
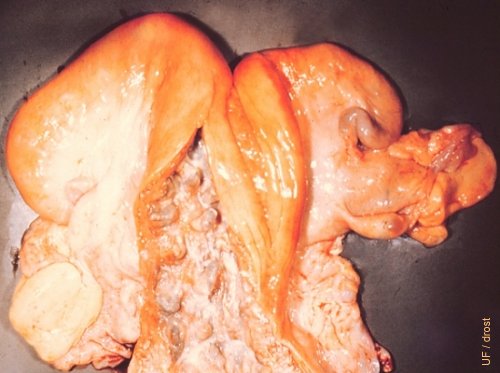
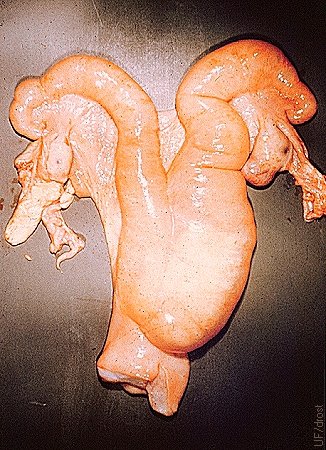
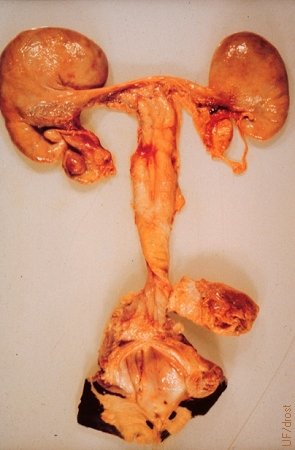
Pluriparous Uterus.
Normal pluriparous uterus. The left horn is the previously gravid horn by virtue of its larger size. A corpus luteum on the right indicates that the cow is cycling.
Thatcher WW (1980)
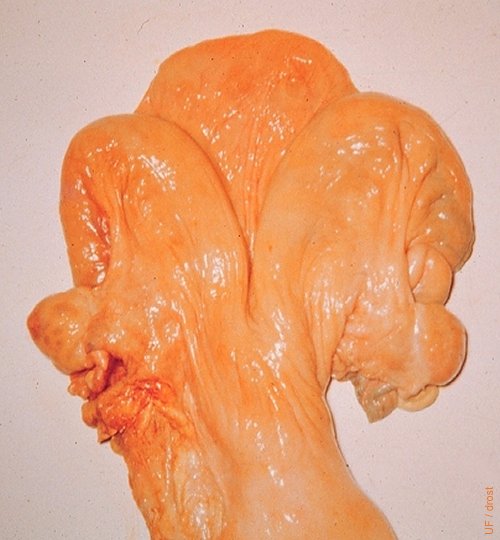
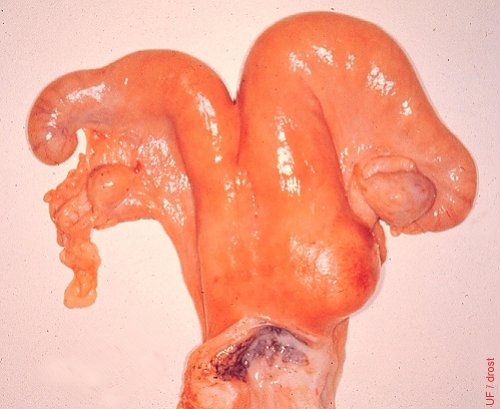
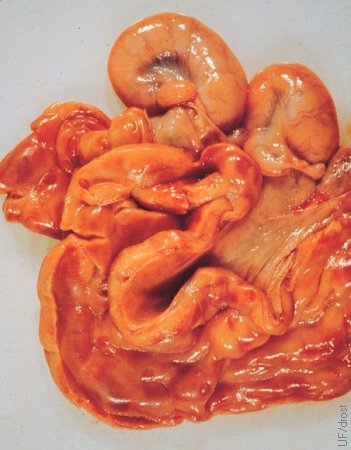
Nulliparous Uterus.
Uterus of a virgin heifer. Note the symmetry of the horns and turgid appearance.
Drost M (1970)

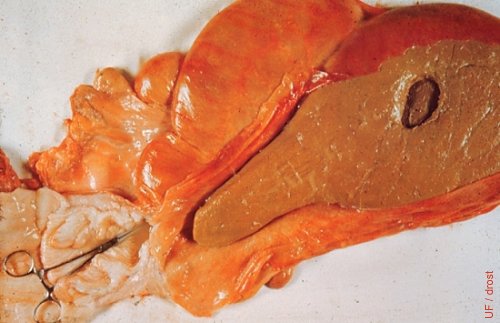
Normal Uterus.
This normal pluriparous uterus is suspended on the sloping surface of a palpation table. The mesovaria are connected rubber bands to hooks, allowing retraction onto the horizontal surface of the table, representing the pelvic floor.
Drost M (1970)
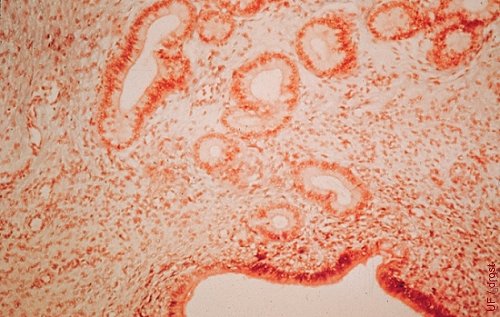
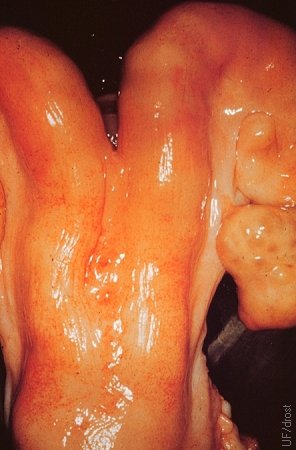
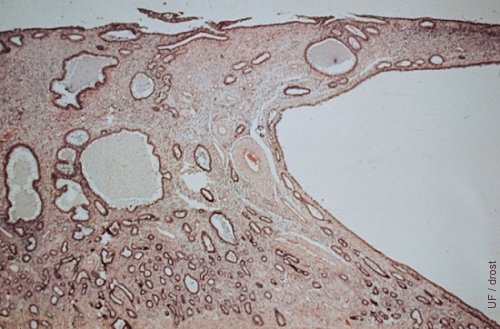
Histology of the Endometrial Glands.
Normal development of the endometrial glands.
Roberts SJ (1973)
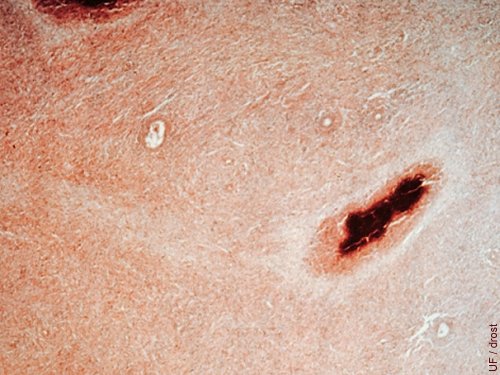
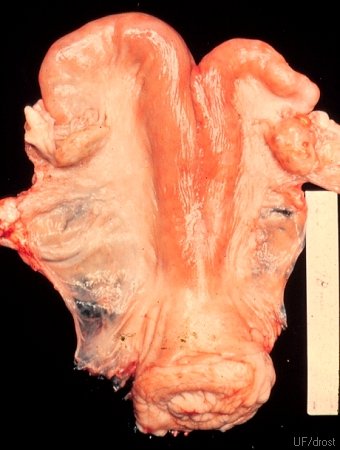
Histology of Avian Tuberculosis.
Avian tuberculous lesion in the endometrium.
Roberts SJ (1973)
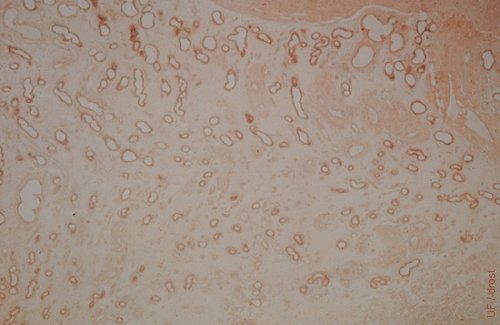
Histology of Cystic Endometrium.
Histopathology of the endometrium showing cystic glands.
Roberts SJ (1973)
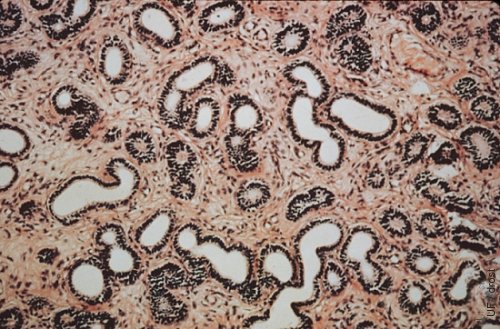
Histology of Mucometra.
Histology of the endometrium of a cow with mucometra.
Roberts SJ (1973)
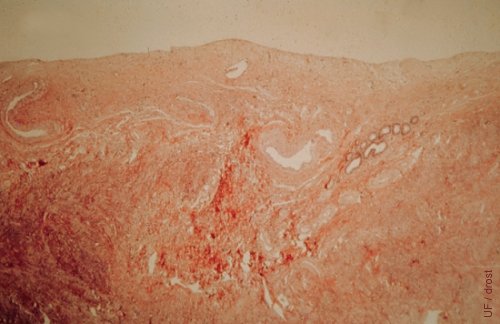
Histology of Cystic Endometrium.
Cystic degeneration of the endometrium of a cow with cystic follicular degeneration.
Roberts SJ (1973)
Sparse Endometrial Glands.
Very few endometrial glands were present in the endometrium of this anestrous heifer. She ovulated but the corpus luteum persisted due to insufficient prostaglandin F2alpha from the endometrial glands.
Drost M (1985)
Lack of Endometrial Glands.
There were no endometrial glands in this heifer. She ovulated but the corpus luteum persisted. No prostaglandin production. Anestrus.
Drost M (1984)

Large Mesonephric Duct Cyst.
A prominent mesonephric duct cyst - a remnant of the male duct system - is present in the intercornual ligament. A rare occurrence.
Roberts SJ (1973)

Small Mesonephric Duct Cyst.
Small mesonephric duct cyst in the prominent intercornual ligament. It is a remnant of the male mesonephric duct system.
Drost M (1974)
Large Edematous Intercornual Ligament.
The intercornual ligament is unusually large and edematous. Etiology unknown.
Roberts SJ (1973)

Serosal Sacculation.
The right horn shows a serosal sacculation, along its greater curvature, which may have formed during the process of involution by entrapment of serosa between the major folds of the uterine wall.
Roberts SJ (1973)
Serosal Cyst.
Contractions of the uterus during postpartum involution causes infolding of the serosa (rugae) which may lead to formation of inclusion cysts.
Drost M (1974)

Utero-rectal Adhesion.
The tip of the right horn was adhered to the rectum due to an old case of perimetritis. The cow was pregnant in the left horn. [the size of the square tile is 15 cm].
Drost M (1974)
Recto-uterine Fistula.
A fistula between the rectum and the right uterine horn led to contamination of the uterus, cervix and vagina with feces. The rectum has been cut away in this postmortem specimen. The contaminated cervical os and the vagina may be seen on the left.
Drost M (1974)

Lochia.
Normal postpartum discharge consisting of blood, mucus and detritus. In the absence of infection it is virtually odor-free.
Morrow DA (1975)

Postpartum Uterus - 12 hours.
Uterus 12 hours after a spontaneous delivery. The fetal membranes were delivered by 8 hours post partum. Note the rugae of a well contracted uterus.
Morrow DA (1975)
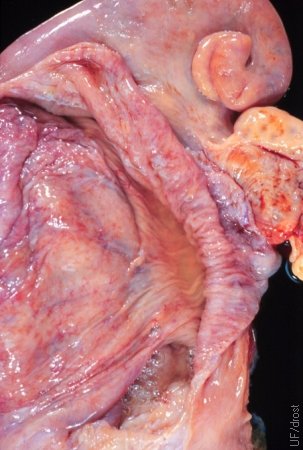
Postpartum Uterine Lumen - 12 hours.
The fetal membranes have detached. The caruncles are denuded.
Morrow DA (1975)

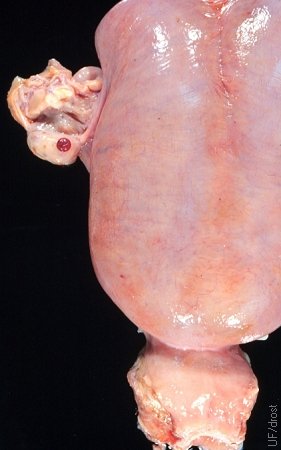
Postpartum Uterus - Day 1.
Large firm uterus with rugae. Cannot be retracted.
Chenoweth PJ (2012)

Postpartum Uterus - Day 5.
Large firm uterus with rugae. Cannot be retracted.
Chenoweth PJ (2012)

Postpartum Uterus - Day 5.
Involuting uterus at 5 days post partum. In the normal cow, firm rugae should be palpable at this stage and there should be no gross accumulation of fluid.
Morrow DA (1975)

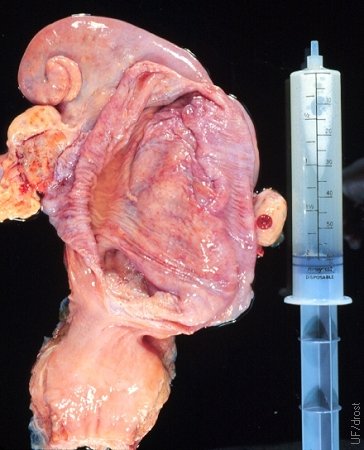
Postpartum Uterine Lumen - Day 5.
The caruncles are denuded. Varying amounts of lochia are still present.
Morrow DA (1975)

Postpartum Uterus - Day 6.
The uterus is thick walled and may contain a considerable amount of normal lochia 6 days after calving.
Morrow DA (1975)

Postpartum Uterine Lumen - Day 9.
Considerable lochia remains. The caruncles have regressed in size.
Morrow DA (1975)

Postpartum Uterus - Day 10.
Firm uterus with rugae. Still cannot be fully retracted by palpation.
Chenoweth PJ (2012)

Involuting Caruncles - Day 10.
Some lochia remains. The caruncles have regressed in size.
Chenoweth PJ (2012)

Postpartum Metritis - Day 10.
The caruncles have regressed in size. Lochia and clotted blood are present.
Chenoweth PJ (2012)
Necrotic Caruncles - Day 10.
The caruncles have regressed in size. Some show evidence of necrosis and infection.
Chenoweth PJ (2012)
Postpartum Uterus - Day 11.
The uterus is thick walled. The ovaries are inactive.
Morrow DA (1975)

Postpartum Uterine Lumen - Day 11.
Normal postpartum uterus on Day 11. Considerable non-odorous lochia may still remain.
Morrow DA (1975)

Postpartum Uterine Lumen - Day 11.
Denuded hemorrhagic caruncles and lochia are present. When infection is present, there may be a foul odor.
Morrow DA (1975)
Postpartum Caruncles - Day 12.
Involuting caruncles in both uterine horns.
Chenoweth PJ (2012)

Postpartum Uterus - Day 14.
Though still somewhat heavy, the uterus is retractable into the pelvic cavity at 14 days post partum.
Morrow DA (1975)

Postpartum Uterus - Day 15.
Distinct asymmetry remains and the uterus is firm. Both ovaries are inactive.
Morrow DA (1975)

Postpartum Uterus - Day 15.
The normal involuting uterus is firm and partially retractable. The horns are asymmetrical. There may be an early follicle.
Chenoweth PJ (2012)
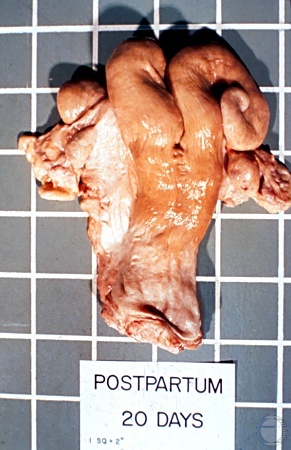
Postpartum Uterus - Day 20.
The normal uterus is 90% involuted by 3 weeks post partum. Ovarian activity has resumed. Some asymmetry remains. The uterus is full retractable.
Chenoweth PJ (2012)

Postpartum Uterus - Day 30.
At 30 days post partum the uterus is generally 95% involuted after a spontaneous vaginal delivery. A fully developed corpus luteum is present on the left ovary.
Morrow DA (1975)

Postpartum Uterus - Day 15 vs Day 30.
The progressive reduction in size over a two-week period can be readily appreciated, when comparing a Day 30 with a Day 15 postpartum uterus.
Morrow DA (1975)

Postpartum Uterine Lumen - Day 30.
At 30 days post partum, the uterine lumen is clean, after a normal vaginal delivery. The caruncles remain prominent.
Morrow DA (1975)
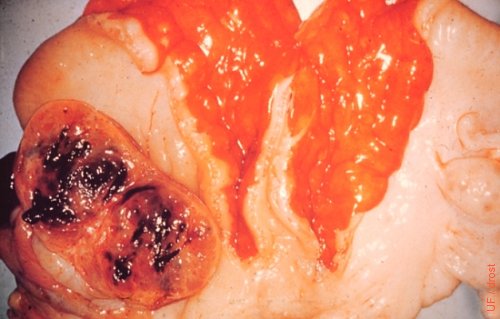
Acute Endometritis.
The acute endometritis was caused by the infusion of Lugol's solution (a 5% aqueous solution of iodine). Incidentally, a corpus luteum had been enucleated, manually per rectum, from the left ovary prior to slaughter.
Seguin B (1976)

Metricheck Instrument.
Vaginal mucus is collected to detect the presence of clinical endometritis.
Santos J (2009)
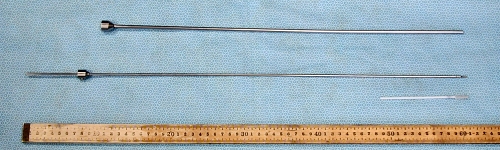
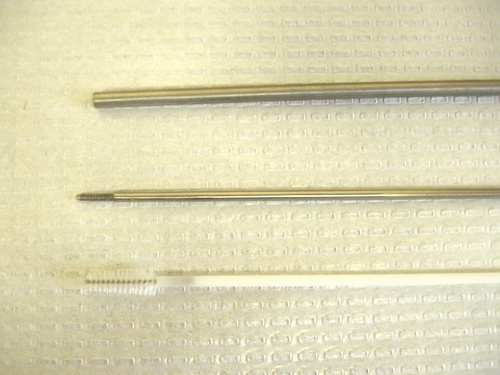
Disassembled Cytobrush Instrument.
At the top, the shaft. In the middle, the plunger (60 cm long). At the bottom on the right, the actual small cytobrush.
Drost M (2010)
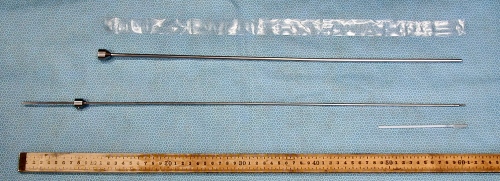
Components of the Cytobrush Instrument.
From the top 1. a sterile sanitary sheath, 2. the shaft, 3. the plunger (60 cm long) 4. the actual cytobrush.
Drost M (2010)

Cytobrush Instrument and AI Syringe.
Comparison of the components of the cytobrush instrument with an assembled standard 0.5 cc artificial insemination syringe (next to the ruler).
Drost M (2010)
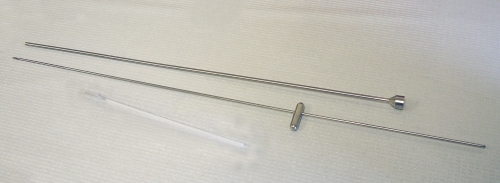
Cytobrush Instrument.
Components of the Cytobrush instrument: the shaft, the plunger, and the Cytobrush proper.
Santos J (2009)
Cytobrush Instrument.
Tips of the components of the Cytobrush instrument: the shaft, the plunger, and the Cytobrush proper.
Santos J (2009)
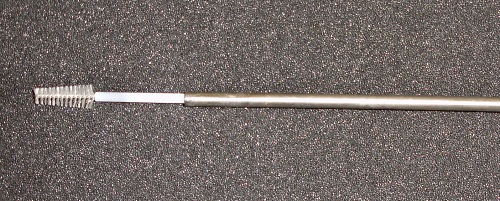
Cytobrush Instrument.
Assembled Cytobrush instrument ready for use.
Santos J (2009)

Sample Collection for Cytology and Culture.
After placement of a sterile Foley catheter and inflation of the balloon, 20 cc of sterile saline are injected into the uterus.
Santos J (2009)

Sample Collection for Cytology and Culture.
After placement of a sterile Foley catheter and inflation of the balloon, 20 cc of sterile saline are injected into the uterus.
Santos J (2009)

Sample Collection for Cytology and Culture.
Withdrawal of the flushing solution. About 15 to 20 cc of the infusate is routinely recovered.
Santos J (2009)

Sample Collection for Cytology and Culture.
Routinely, about 80% of the amount of fluid infused is recovered.
Santos J (2009)

Sample Collection for Cytology and Culture.
The uterine sample is placed in a sterile centrifuge tube.
Santos J (2009)
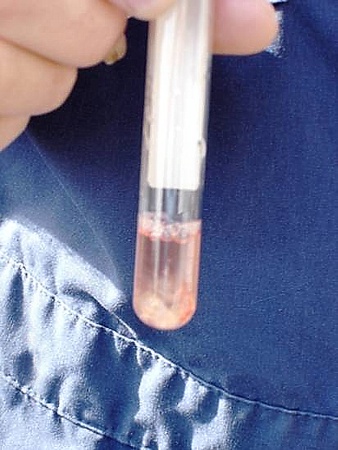
Sample Collection for Cytology and Culture.
Some flocculent material is evident in the bottom of the tube. The pink color is due to the presence of some blood in the fluid.
Santos J (2009)

Sample Collection for Cytology and Culture.
Culturing the uterine sample by streaking it on a blood agar plate.
Santos J (2009)
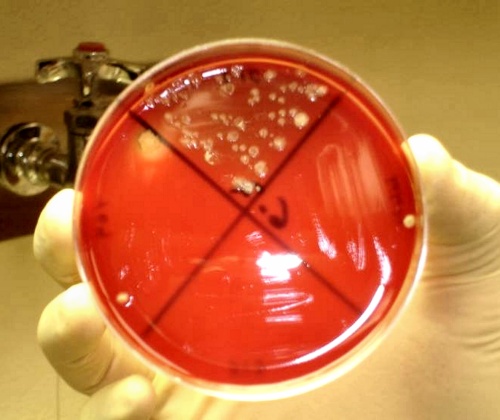
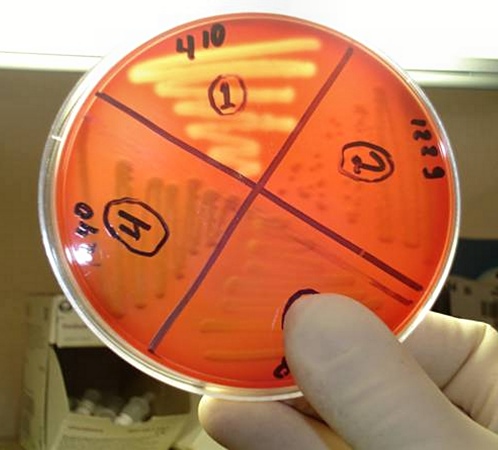
Culture Results.
Of the four samples from different cows in the quadrants, the bottom one showed no growth. The other three showed bacterial growth on the blood agar plate.
Santos J (2009)

Culture Results.
Four samples of uterine flush. Growth in all four quadrants.
Santos J (2009)
Culture Results.
Four samples. Growth in all four quadrants of a blood agar plate. There is evidence of bacterial growth in the upper quadrant.
Santos J (2009)

Stained Endometrial Smears.
Endometrial smears for cytology stained with Diff Quick (Romanowsky stain). Samples are fixed in methyl alcohol and then stained sequentially in eosin and azure solutions.
Santos J (2009)
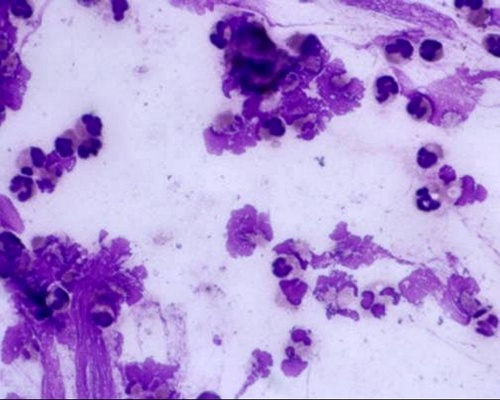
Endometrial Cytology Results.
Presence of an abundant number of polymorphonuclear leukocytes (small dark stained cells) and endometrial cells (pink cytoplasm and large round nucleus).
Santos J (2009)
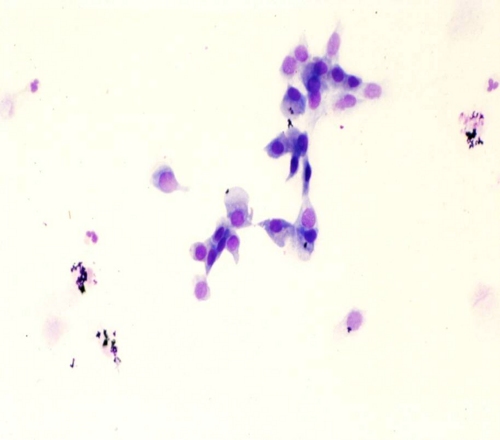
Endometrial Cytology Results.
Normal endometrial cytology. Presence of endometrial cells in the absence of neutrophils.
Santos J (2009)
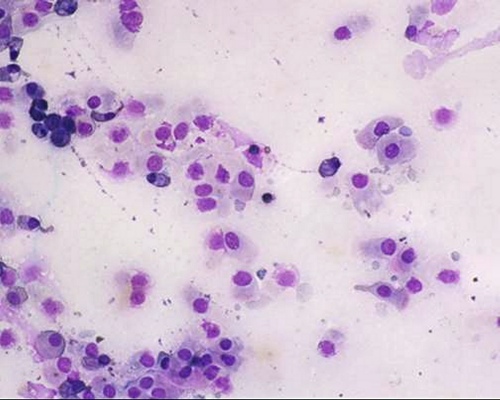
Endometrial Cytology Results.
Endometrial cells and occasional polymorphonuclear leukocytes.
Santos J (2009)

Cervical Discharge.
Cervical discharge of mucopus indicating either a uterine or a cervical infection.
Roberts SJ (1973)
Metritis.
The left horn is thick walled. Pus is present in the lumen. The caruncles are poorly involuted.
Drost M (1970)
Pathognomonic Pipet Abscess.
The location of the spherical abscess at the base of the right horn is highly suggestive of a pipet abscess. When a treatment pipet is passed through the cervix it is relatively easy to perforate the uterine wall anterior to the internal os of the cervix, especially in an infected uterus. Contamination from the lumen then directly invades the wall. The endometrium may heal over the area and create a firm localized abscess.
Drost M (1970)

Inspissated Necrotic Caruncles.
Chronic postpartum metritis. Disintegrating, inspissated necrotic caruncles are still present.
Drost M (1974)

Inspissated Necrotic Caruncles.
Considerable involution of the uterus has occurred. However, the lumen contains inspissated necrotic caruncular material.
Roberts SJ (1973)
Inspissated Uterine Secretions.
The lumen of the right horn does not communicate with the lumen of the body of the uterus and the cervix. The trapped secretions became inspissated over time. Ultimately this can lead to the formation of a uterolith.
Drost M (1974)

Dried Uterine Secretions.
This opened uterus shows some dried uterine secretions as well as cystic endometrial hyperplasia.
Drost M (1974)

Dried Uterine Secretions.
The dried uterine secretions have been lifted out of the lumen. The endometrium is clean but shows multiple cysts, likely due to prolonged elevated estrogen levels.
Drost M (1974)

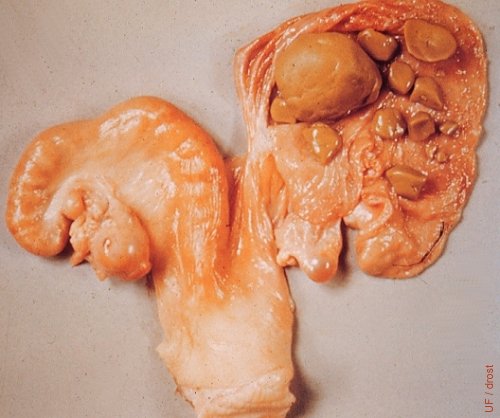
Hysteroliths.
Hysteroliths, or uterine stones, are present in both horns in this slaughterhouse specimen. They are the result of inspissation of uterine secretions trapped in the lumen because of an obstruction.
Drost M (1974)
Uterine Stones.
Segmental hypoplasia of the right horn of the uterus has led to the inspissation of the trapped uterine secretions. The mass subsequently broke up into smaller fragments, called hysteroliths or uterine stones. This cow cycled normally; notice CL on the left ovary. A follicle is present on the right ovary. Ovulation from the ovary ipsilateral to the incomplete horn would lead to a persistent CL due to the lack of prostaglandin F2alpha.
Roberts SJ (1973)

Segmental Uterine Aplasia.
Segmental hypoplasia of the left horn of the uterus has led to the inspissation of the trapped uterine secretions, and the formation of hysteroliths. [The normal ovaries were removed for the IVF laboratory from this random slaughterhouse specimen].
Drost M (2009)

Segmental Aplasia.
Segmental hypoplasia of the left horn of the uterus has led to the inspissation of the trapped uterine secretions, and the formation of inspissated uterine secretions and two hysteroliths. [The normal ovaries were removed for the IVF laboratory from this random slaughterhouse specimen].
Drost M (2009)

Segmental Aplasia.
Segmental hypoplasia of the left horn of the uterus has led to the inspissation of the trapped uterine secretions, and the formation of inspissated uterine secretions and two hysteroliths. The occluded tip of the left horn has been opened to show its contents.
Drost M (2009)

Isolated Tip of Uterine Horn.
Segmental hypoplasia of the left horn of the uterus has led to the inspissation of the trapped uterine secretions, and the formation of inspissated uterine secretions and two hysteroliths. Close-up of opened tip of the horn.
Drost M (2009)

Hysterolith - Close-up.
Close-up of a 4.0 x 3.0 x 1.5 cm uterine stone, from an occluded tip of the left horn in a cow with segmental uterine aplasia. The consistency of this stone was crumbly. They become firmer with age.
Drost M (2009)

Removal of a Foreign Body.
Restraint of the cow for colpotomy and removal of a foreign body from the lumen of the uterus.
Drost M (2009)

Foreign Body Removal.
Foreign body removal such as a broken tip of a Cytobrush, or a hysterolith, can be done by colpotomy. The cow is prepared for aseptic surgery under epidural anesthesia.
Drost M (2009)
Foreign Body.
Ultrasound image of the broken tip of a Cytobrush at the base of the uterine horn. This foreign body (corpus alienum) was removed via colpotomy.
Drost M (2009)

Colpotomy Procedure.
Introduction of the colpotomy spear under aseptic conditions and epidural anesthesia.
Drost M (2009)

Removal of Foreign Body.
Extraction of a 7.5 cm broken off piece of the tip of a Cytobrush, after pushing it through the wall of the uterus.
Drost M (2009)

Foreign Body.
A bloody, 7.5 cm, broken off piece of the tip of a Cytobrush, retrieved via colpotomy.
Drost M (2009)

Foreign Body.
A clean 7.5 cm broken off piece of the tip of a Cytobrush, retrieved via colpotomy.
Drost M (2009)

Uterus After Retrieval.
A small puncture wound is visible after retrieval of the brush tip from the lumen of the uterus.
Drost M (2009)

Closure of the Uterus.
A finger hole was made into the uterine lumen to locate the lost catheter tip. The hole was closed with a Utrecht pattern. An assistant was required to hold the uterus for the surgeon.
Drost M (2009)

Closed Incision.
The exploratory hole into the uterine lumen, to locate the lost catheter tip, has been closed with a Utrecht pattern.
Drost M (2009)

Closed Incision Close-up.
The exploratory hole into the uterine lumen, to locate the lost catheter tip, has been closed with a Utrecht pattern.
Drost M (2009)

Chronic Metritis.
Chronic unilateral metritis in the right horn in a cow 40 to 50 postpartum. The left horn has involuted normally; the endometrium is clean. The cow was sent to slaughter 4 days after her second heat. Note corpus luteum on the right ovary.
Roberts SJ (1973)

Pyometra.
Classical bovine pyometra. The uterus contained several liters of pus which could be moved from horn to horn by compression of the horns. A persistent corpus luteum was present and the cervix was closed [each square tile measures 15 cm].
Drost M (1970)
Postcoital Pyometra.
Postcoital pyometra is pathognomonic for trichomoniasis in cattle.
Drost M (1980)

Postcoital Pyometra.
Postcoital pyometra is pathognomonic for trichomoniasis in cattle.
Drost M (1980)
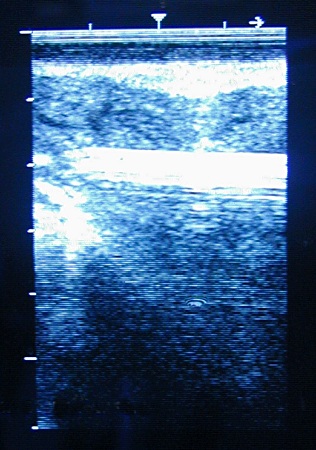
Ultrasonography of Pyometra.
Pyometra in the cow manifests itself by the accumulation of pus in the uterus while the cervix is closed and the corpus luteum is maintained, with the result that the cow is anestrous. The cow is not systemically ill. On palpation per rectum the fluid can be made to move from one horn to another, in contrast with a gravid uterus of comparable size. There are no positive signs of pregnancy such as a membrane slip, presence of an amniotic vesicle or fetus or caruncles.
Pieterse MC (1999)
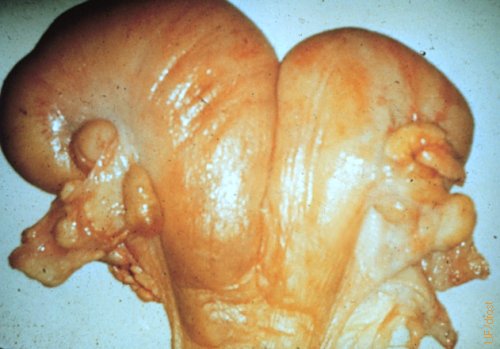
Mucometra.
Adhesion of the cervix causing obstruction and secondary mucometra. The adhesion is a result of trauma.
Roberts SJ (1973)

Mucometra.
The white scar caused a cervical obstruction which lead to secondary mucometra.
Roberts SJ (1973)

Imperforate Hymen and Mucometra.
Congenital imperforate hymen is rare in cattle. The complete blockage results in accumulation of uterine and cervical secretions and formation of mucometra, mucocervix, and mucovagina . Note the corpus luteum. Cows and heifers with mucometra or hydrometra generally cycle normally in contrast to cows with pyometra that are anestrous for long periods of time. [the size of the square tile is 15 cm].
Roberts SJ (1986)
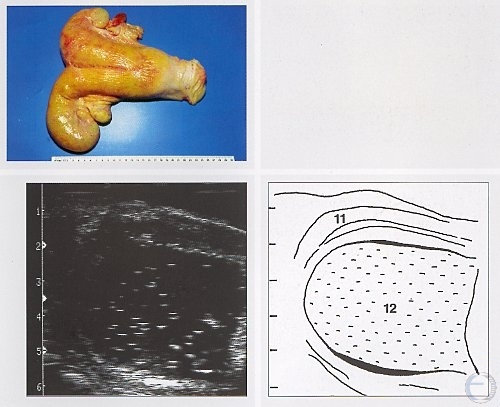
Hydrometra.
Fluctuant thin walled uterus with hydrometra as a result of occlusion by an anomalous cervix.
Roberts SJ (1973)

Hydrometra.
Hydrometra due to an obstruction near the internal os of the cervix. Both horns and the body of the uterus are distended with fluid. The uterus is thin walled. The uterus contained 5 liters of watery fluid.
Roberts SJ (1973)

Hydrometra.
Hydrometra is generally the result of an obstruction. In this instance the blockage is at the level of the cervix. The right horn and the body of the uterus are distended with watery fluid.
Drost M (1971)
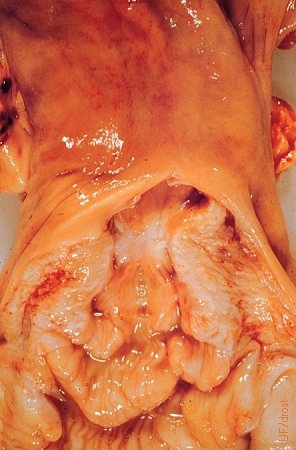
Hydrometra / Endometrium.
The endometrium of the thin-walled uterus of a cow with hydrometra shows a normal gross appearance, like that of a non-gravid uterus.
Drost M (1971)
Hydrometra / Clear Fluid.
Clear watery fluid was aspirated from the lumen of the uterus with hydrometra. The cow was cycling as documented by the Day 3 corpus hemorrhagicum on the right ovary. Cows with pyometra do not cycle, while cows with a hydrometra do.
Drost M (1971)
Bilateral Hydrometra.
Both horns are distended with fluid indicating that an obstruction must be present at the level of the cervix. The uterus is thin walled and the fluid can be displaced manually per rectum from horn to horn, in contrast with the fluids of a pregnant uterus. The young corpus hemorrhagicum indicates that the cow was recently in heat.
Drost M (1971)
Unilateral Hydrometra.
While not readily discernible, there must be an occlusion at the base of the left horn trapping the uterine secretions in the horn. An incidental follicular cyst is present on the right ovary.
Drost M (1971)

Imperforate Hymen.
Imperforate hymen is a rare condition that causes great distension of the vagina by mucus. In this necropsy specimen, the thin, stretched vaginal has been opened. Heifers with an intact hymen will cycle normally, but intromission by penis or pipet is not possible. [size of the square tile is 15 cm].
Roberts SJ (1973)

Cystic Endometrial Hyperplasia.
Cystic endometrial hyperplasia may develop after chronic exposure to estrogens such as phytoestrogens or estrogenic implants. It may also be a sequella to chronic cystic follicular degeneration or granulosa cell tumors. In this slaughterhouse specimen a fully developed corpus luteum is present on the right ovary.
Drost M (1971)
Cystic Endometrial Hyperplasia.
Cystic endometrial hyperplasia may develop after chronic exposure to estrogens such as phytoestrogens or estrogenic implants. It may also be a sequela to chronic cystic follicular degeneration or granulosa cell tumors. In this slaughterhouse specimen, the right horn has been opened to show the hyperplastic endometrial cysts and some inspissated secretions.
Drost M (1971)
Cystic Endometrial Hyperplasia.
Cystic endometrial hyperplasia may develop after chronic exposure to estrogens such as phytoestrogens or estrogenic implants. It may also be a sequela to chronic cystic follicular degeneration or granulosa cell tumors. In this slaughterhouse specimen, the right horn has been opened to show the hyperplastic endometrial cysts. Inspissated secretions were pulled from the lumen and are shown above the tract.
Drost M (1971)

Bilateral Cystic Endometrial Hyperplasia.
Cystic endometrial hyperplasia may develop after chronic exposure to estrogens such as phytoestrogens or estrogenic implants. It may also be a sequela to chronic cystic follicular degeneration or granulosa cell tumors. In this slaughterhouse specimen, the uterine lumen has been exposed to show the hyperplastic endometrial cysts.
Drost M (1971)

Bilateral Cystic Endometrial Hyperplasia.
Cystic endometrial hyperplasia may develop after chronic exposure to estrogens such as phytoestrogens or estrogenic implants. It may also be a sequela to chronic cystic follicular degeneration or granulosa cell tumors. In this slaughterhouse specimen, both uterine horns have been opened and rinsed to show the hyperplastic endometrial cysts.
Drost M (1971)
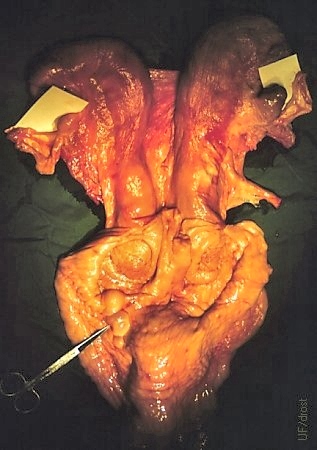
Uterus Didelphys.
In a rare true double cervix, or uterus didelphys, there are two cervices each connected to its respective uterine horn. The scissors are pointing to two mesonephric duct cysts (Gartner's ducts), remnants of the male duct system.
Goemann GG (1975)

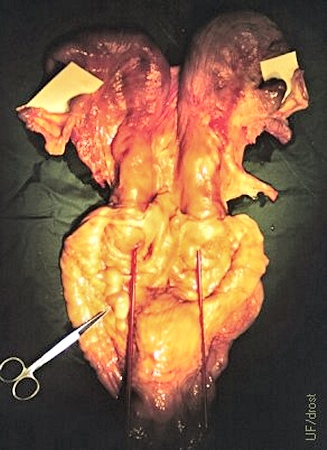
Uterus Didelphys.
In a rare true double cervix, or uterus didelphys, there are two cervices each connected to its respective uterine horn. In this ventral view a septum is visible between the two cervices as delineated by a red pipet.
Goemann GG (1975)
Uterus Didelphys.
In a rare true double cervix, or uterus didelphys, there are two cervices each connected to its respective uterine horn. A red pipet is inserted in each of the two cervical canals. Gartner's ducts are indicated by the scissors.
Goemann GG (1975)
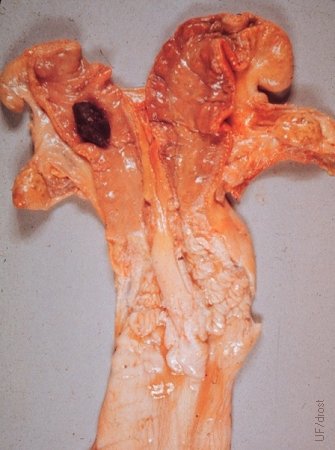
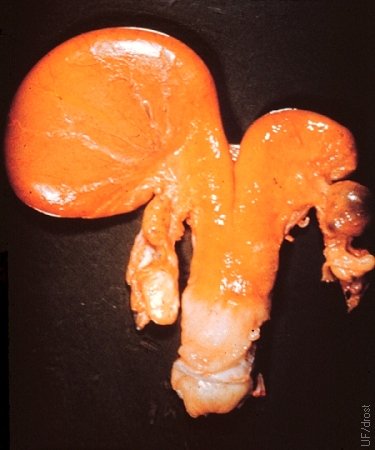
Uterus Didelphys with Hysterolith.
Segmental aplasia of the left uterine horn and complete duplication of the cervix (uterus didelphys). There is an occluding obstruction at the base of the left horn which trapped uterine secretions. Here the secretions are inspissated and have formed a hysterolith (uterine stone; uterine "pebble" in this case?). The corpus luteum is retained for lack of a signal from the ipsilateral horn (prostaglandin F2alpha) to regress. The cow appears to have been pregnant in the right horn.
Roberts SJ (1973)

Segmental Hypoplasia.
The base of the right horn is missing. Uterine secretion have accumulated in the isolated portion of the horn. When such animal ovulates from the ovary ipsilateral to the incomplete horn, the corpus luteum persists due to lack of a lutelolytic prostaglandin signal from the defective horn. The animal can conceive on the intact size.
Tanabe TY and Almquist GO (1966)

Segmental Hypoplasia.
The base of the right horn is missing. Uterine secretion have accumulated in the isolated portion of the horn. When such animal ovulates from the ovary ipsilateral to the incomplete horn, the corpus luteum persists due to lack of a lutelolytic prostaglandin signal from the defective horn. These animals can conceive on the intact size. This tract came from a prepuberal heifer.
Drost M (1970)
Bilateral Segmental Hypoplasia.
Bilateral segmental hypoplasia in an 18-month old heifer. The isolated portions of the horns contained mucus (mucometra). Her twin sister had a uterus unicornis.
Roberts SJ (1973)

Multiple Hypoplasia.
While present, the left horn is incomplete and does not connect with the cervix. Trapped secretions have become inspissated. The right uterine tube (oviduct) is also incomplete and ends in a cystic structure, a rare anomaly. (Slide donated by Dr. A de la Concha).
Drost M (1985)

Uterus Unicornis.
Congenital absence of the right horn. Segmental aplasia of the paramesonephric duct. Both ovaries are present and functional. However, when ovulation occurs on the ovary unaccompanied by a horn the corpus luteum fails to regress due to lack of a uterine luteolysin. The right ovary displays an old scar after digital enucleation of the CL, per rectum, as a treatment aimed at terminating the anestrus. Unilateral ovariectomy can be used as a management approach.
Roberts SJ (1973)

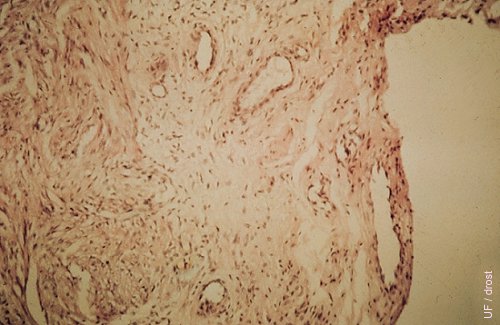
Uterine Tuberculosis.
Granulomatous lesions are present in the endometrium of the right horn. (Slide donated by Dr. A de la Concha).
Drost M (1985)

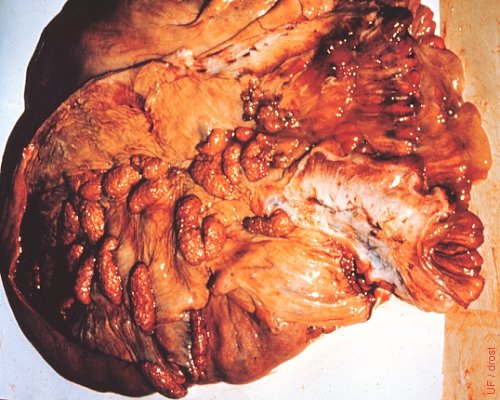
Lymphosarcoma of the Uterus.
Lymphosarcoma of the uterus. Numerous smooth round firm tumors could be palpated in the uterine wall. The neoplastic growths followed the vascular supply of the caruncles.
Roberts SJ (1973)
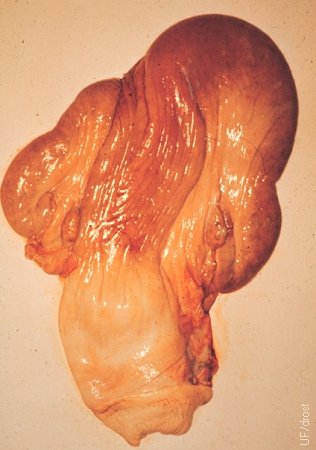
Lymphosarcoma of the Uterus.
Lymphosarcoma of the uterus. Note the thickened, firm uterine wall.
Drost M (1971)

Lymphosarcoma of the Uterus.
Smooth firm masses could be palpated in the wall of the uterus.
Drost M (1971)

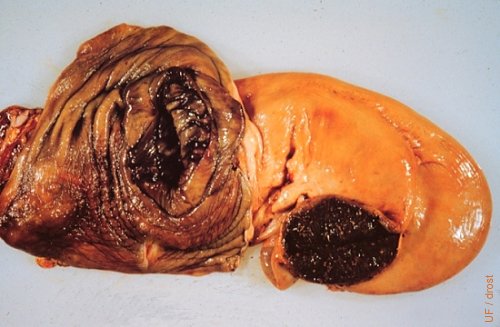
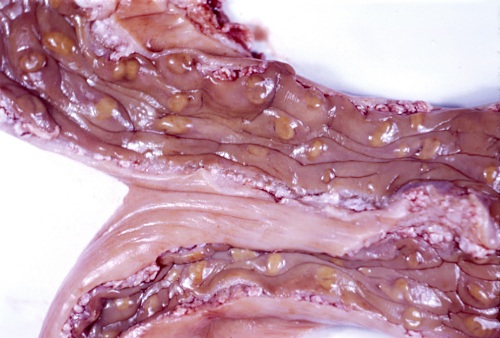
Lymphosarcoma - Cross-section.
A cross section of the uterine horn shows the thickened wall due to lymphosarcoma. The rate of development of lymphosarcoma is generally rapid.
Drost M (1971)

Leiomyoma.
Leiomyomas generally occur as a solitary growth in the wall of the uterus. Because of their firmness and smoothness that can be confused with an abscess, on palpation. For orientation, notice an inactive ovary at the bottom right of the image. Also visible are numerous involuted caruncles in the opened lumen of the uterus, indicating that this was the uterus of a pluriparous cow. This was an incidental slaughterhouse specimen.
Drost M (1980)

Fat Necrosis.
Necrosis of the mesenteric fat can be extensive. Saponification of the fat renders it firm (like a bar of soap). It may be mistaken for a fetus. In this illustration the fat encroaches on the lumen of the intestines which may lead to obstruction. It has been associated with heavily fertilized fescue pastures.
Drost M (1971)