The Visual Guide to
Bovine Reproduction
- Normal Calving
- Multiple Births
- Calving Facilities
- Pelvic Dimensions
- Calving Problems
- True Breech
- Sizing the Fetus
- Calving Injuries
- Cesarean Section
- Fetotomy
- Pelvic Splitting
- Episiotomy
Obstetrics: Calving Problems
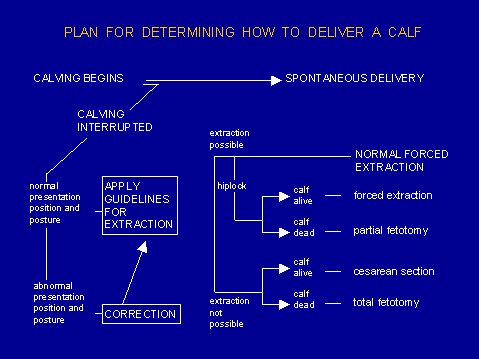
Calving Plan.
This systematic plan for dealing with the delivery of a calf was developed in the obstetrical clinic of the Faculty of Veterinary Medicine of Utrecht University in The Netherlands. The plan stresses that assisted delivery of a calf is not a trial-and-error procedure. Valuable time can be saved, and unnecessary trauma to the cow and the calf can be prevented by following this flow chart.
Schuijt G and Ball L (1980)

Supplies Needed.
Bucket, water, soap, lubricant, chains and handles, stomach pump and stomach tube, vaseline jar.
LeBlanc MM (2013)

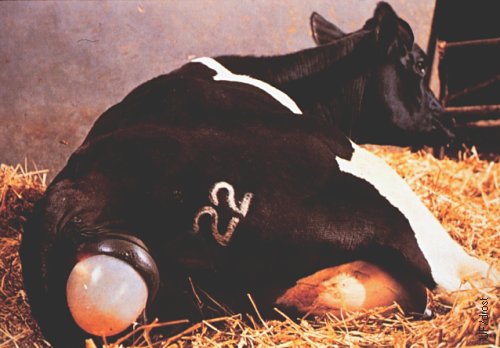
Early Labor - Amnion Intact.
This cow is in early labor. The chorio-allantois has ruptured and now the blueish-gray intact amnion is showing, containing two hooves.
Drost M (1976)
Early Labor - Amnion Showing.
The blue-gray amnion is showing in this cow during the early part of labor. The fluid-filled membranes aid in dilation of the cervix and birth canal. The amniotic fluid will serve as lubrication once the amnion ruptures.
Drost M (1976)
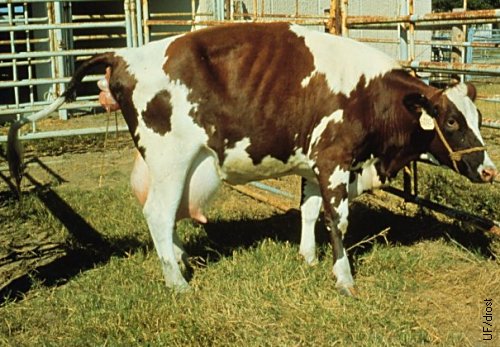
Early Labor - Foot Showing.
This Red Holstein heifer is in active labor. The membranes have ruptured and a foot is showing. Note the distended udder and turgid teat.
Drost M (1982)

Stage 2 of Labor.
Labor in this Red Holstein heifer is progressing nicely. The calf is in anterior presentation, dorso-sacral position, with normal posture. Both pasterns appear to extend 15 cm or more beyond the vulva, indicating that the shoulders have passed through the critical bony pelvic inlet. This further indicates that there is enough room for the fetal hips to pass between the iliac shafts.
Drost M (1982)
Normal Anterior Presentation.
This is stage 2 of labor. The cervix is fully dilated. The calf is in normal anterior longitudinal presentation, in normal dorso-sacral position, and with normal posture (both legs and head and neck extended).
Drost M (1974)
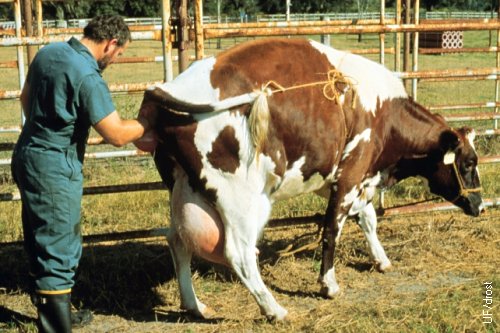
Obstetrical Examination.
The veterinarian is in the process of a direct obstetrical examination per vaginam, to determine if the cervix has fully dilated, as well as the presentation, position and posture of the calf, plus whether the calf is alive or not.
Haibel GK (1983)

Vestibulo-Vaginal Trauma.
Severe, nearly complete constriction of the vagina at the level of vulvo-vaginal junction (hymen) in a pluriparous cow. The calf was dead, the cervix dilated, and there was a foul odor with staining of the vagina on the left. [Bladder and urethra in the lower left corner].
Gunn A (2010)

Vestibulo-Vaginal Stricture.
Severe constriction of the vagina at the level of vulvo-vaginal junction leaving an aperture of less than 1 cm. Vulva is in the upper right hand corner. The stained vagina is due to foul discharge from the uterus. The cow had delivered a calf before (per vaginam) and may have been traumatized at that time. The incised tissues of the roof of the vestibulum are white. The cow had been artificially inseminated.
Gunn A (2010)

Minimal Obstetrical Supplies.
Minimal supplies needed: Bucket, water, Vaseline, soap, lubricant, two short chains (75 cm), one long chain (150 cm), and two handles.
Drost M (2009)

Obstetrical Supplies.
Obstetrical supplies: Bucket, water, Vaseline, soap, lubricant, two handles, short chains (75 cm), one long chain (150 cm), and a stomach pump and tube for colostrum feeding.
Drost M (2009)

Epidural Anesthesia 1.
Selecting the injection site, the first movable saccro-coccygeal space, by moving the tail up and down and feeling for a depression.
Prado TM (2007)

Epidural Anesthesia 2.
Placement of the needle. The hub of the needle should be angled slightly posteriorly. Clipping and surgical preparation of the injection site are preferred by most veterinarians.
Prado TM (2007)

Epidural Anesthesia 3.
Correct placement of the needle may be tested by placing a drop of anesthetic fluid on the hub of the needle. When placed correctly, the drop will be aspirated. If the drop is not aspirated, the correct placement may be further tested by gauging the ease with which the plunger can be compressed, preferably by using the index finger.
Prado TM (2007)

Epidural Anesthesia 4.
Injection of the anesthetic solution should be easy, with minimal resistance.
Prado TM (2007)
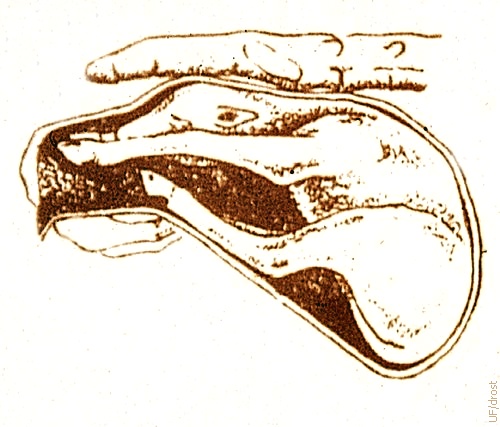
Anterior Presentation; Closed Cervix.
Most calves are born in anterior, longitudinal presentation and are carried that way for the latter part of gestation. It is unlikely that the fetus is capable of changing its orientation from cranial to caudal after the fifth month of gestation when the fetus has attained the size of a large cat and when there is insufficient room for the fetus to turn around in utero.
Drost M (1974)
Normal Anterior Longitudinal Present'n.
Calf is in anterior longitudinal presentation (head first), dorso-sacral position (right side up), and has normal posture (both limbs and head and neck extended).
Utrecht (1976)

Early Labor.
Water bag has broken. Onset of Stage 2, expulsion of the calf.
Smith MC (2013)

Active Labor.
One foot showing. Active labor. Time to determine presentation, position, and posture.
Smith MC (2013)

Active Labor.
Second foot showing. Continued labor. Time to determine presentation, position, and posture.
Smith MC (2013)

Assisted Delivery.
Two feet and the nose of the calf are presented. Traction provided in synchrony with the straining of the cow.
Smith MC (2013)

Assisted Delivery.
Two feet and the muzzle of the calf are presented. Tongue protrudes under pressure. Traction provided in synchrony with the straining of the cow.
Smith MC (2013)

Immediately Post Partum.
Fresh blood is normal right after delivery. Some may come from the ruptured umbilical cord, some from superficial mucosal tears in the vagina and vestibule.
Smith MC (2013)


Left Leg Retained at Carpus.
Retention of one or both legs at the carpus / carpi makes the diameter of the fetus too large for passage through the birth canal.
Utrecht (1976)
Correction of Retained Carpus 1.
If the calf is not too large, retention at the carpus can be corrected by grasping the metacarpus and by directing the carpus upward and laterally, while turning the hoof medially and in extension of the leg.
Drost M (1976)
Correction of Retained Carpus 2.
If the calf is large, or if there is limited room to maneuver, a chain or a rope may be placed on the distal portion of the limb and traction applied to it while the carpus is repelled upwards and laterally.
Drost M (1976)
Left Leg Retained at the Shoulder.
Retention of one or both legs at the shoulder makes the diameter of the fetus too large for passage through the birth canal.
Utrecht (1976)

Repelling the Shoulder.
Correction of the abnormal posture due retention of the limb at the shoulder must start by repelling the calf to create more room for maneuvering and subsequent recovery of first the carpus, and then the foot.
Utrecht (1976)
Repelling the Calf.
Further repulsion of the calf to gain access to the carpus and the foot, for correction of the abnormal posture.
Utrecht (1976)
Retrieving the Carpus.
The humerus is grasped and the carpus is twisted medially.
Utrecht (1976)
Pulling the Carpus Upwards.
The carpus is lifted up and directed medially while so the distal part of the forelimb can be reached and extended.
Utrecht (1976)

Elevating the Pastern.
While the metacarpus is grasped firmly, the carpus is directed upwards and laterally to guide the pastern medially.
Utrecht (1976)

Pushing Carpus Upwards and Laterally.
While the metacarpus is grasped firmly, the carpus is twisted upwards and laterally to lift the claw above the level of the pubic brim.
Utrecht (1976)
Cupping the Claws.
It is important to protect the tight ventral wall of the uterus just below the pubic brim against the pointed claw by cupping the hand around the hooves.
Utrecht (1976)
Posterior Longitudinal Presentation.
This calf is in a posterior longitudinal presentation (backwards), dorsosacral position, and normal posture (both legs extended).
Utrecht (1976)

Repelling Posterior Presentation.
This calf is in a posterior longitudinal presentation, dorsosacral position, with the right leg retained at the hock. The calf is being repelled (pushed back) into the uterus to make room for maneuvering the leg into extension.
Utrecht (1976)
Repositioning the Hock.
The hock is pushed upwards and laterally to make the hoof accessible to the obstetrician.
Utrecht (1976)
Repositioning the Hock.
The hock is pushed upwards and laterally to make the hoof accessible to the obstetrician.
Utrecht (1976)

Repelling Hock while Pulling on Foot.
With a chain attached to the foot, the hock is pushed anterio-laterally while the leg is extended by pulling on the fetlock.
Utrecht (1976)

Cupping the Claw.
The uterine wall is protected against the pointed claws by cupping them with the hand.
Utrecht (1976)
Final Extension of the Leg.
Both legs are now extended, reducing the diameter of the calf. The next step is to measure the relative size of the calf and the amount of space in the pelvic cavity.
Utrecht (1976)

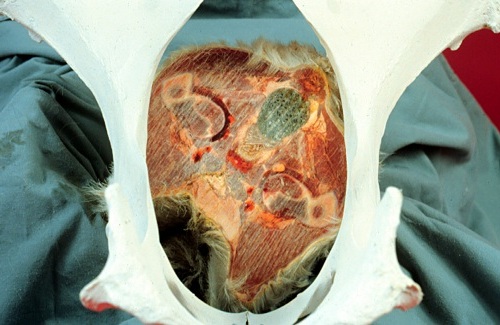
Transverse Dorsal Presentation.
With a transverse dorsal presentation the back of the calf is presented towards the pelvic inlet. The head and the forelimbs are in one horn, the hindlimbs in the opposite horn. It is extremely difficult for the obstetrician to get a hold of any portion of the calf. Furthermore, dilation of the birth canal is poor due to the absence of extremities in the areas of the cervix and the vagina. This presentation is fortunately rare and calls for cesarean section. [size of the square tile is 15 cm].
Drost M (1976)

Twins.
The twin on the left is in anterior longitudinal presentation and its right leg is retained. The twin on the right is in posterior longitudinal presentation with both legs extended. To differentiate a front leg from a hind leg count the number of joints below the hock or the elbow, which feel similar inside the cow. There are two joints below the elbow and there is only one joint below the hock. It is usually advisable to deliver the twin in posterior presentation first.
Drost M (1976)
Transverse Ventral Presentation.
A transverse ventral presentation is extremely rare due to the anatomical configuration of the bicornuate uterus of the cow. A transverse ventral presentation occurs with a Schistosomus reflexus fetal monster when the externalized fetal viscera are presented in the birth canal and the fetal limbs are directed anteriorly due to the extreme flexion of the vertebral column in the lumbar area.
Drost M (1976)

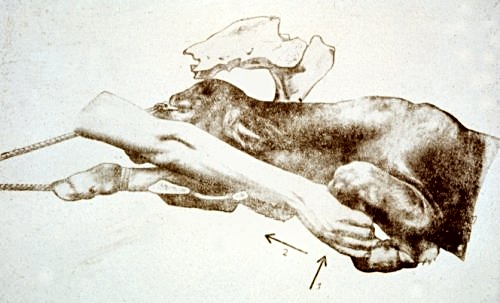
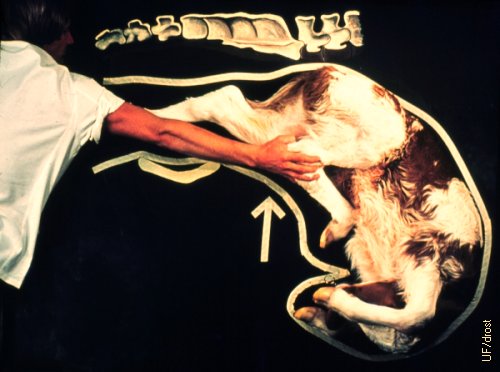
Left Lateral Deviation of the Head.
The calf is in anterior longitudinal presentation, dorso-sacral position, with its head deviated to the left (of its own body). This abnormal posture is frequently the result of a weak fetus or dead fetus that fails to participate in the delivery process by keeping its head and neck extended.
Drost M (1976)
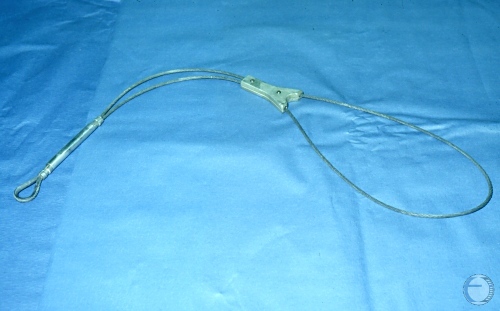
Head Snare.
Adjustable head snare used to retrieve retained fetal parts.
LeBlanc MM (2013)

Eye Hooks.
Eye hooks to insert into the medial canthi of the eye sockets. This method is used to pull the head into the birth canal.
QuIdee GmBH (2013)

Eye Hooks in Place.
Eye hooks in place. The yellow rope pulls the hooks together and the head can now be directed into the birth canal.
QuIdee GmBH (2013)

Alignment of the Head.
Eye hooks in place. The yellow rope pulls the hooks together and the head can now be directed into the birth canal.
QuIdee GmBH (2013)

Head Only Presentation.
The calf in this Charolais cow is in anterior longitudinal presentation, dorso-sacral position and both front limbs are retained at the shoulders. The head is swollen due to blockage of both jugular veins. It cannot be repelled. Solution: decapitation by fetotomy.
Villarroel A (2013)
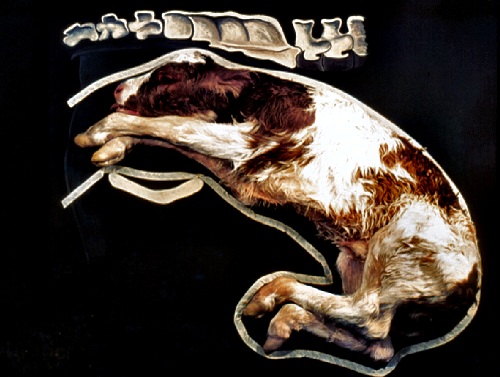
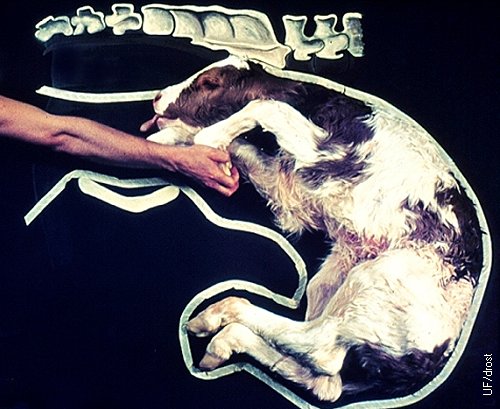
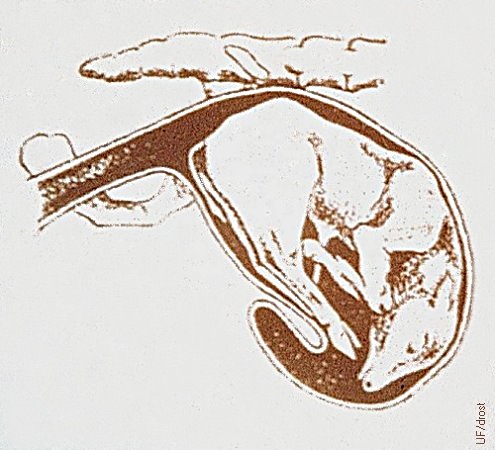
Dogsitting Position.
The dog sitting position is a descriptive term for a fetus in anterior presentation, and dorso-sacral position, whose hind legs are extended and enter the pelvic inlet. Correction is very difficult unless the front half of the fetus can be repelled and the fetus extracted by the hind legs. Traction on the front limbs with partially repelled hindlimbs can result in perforation of the uterine wall below the pubic brim.
Drost M (1976)

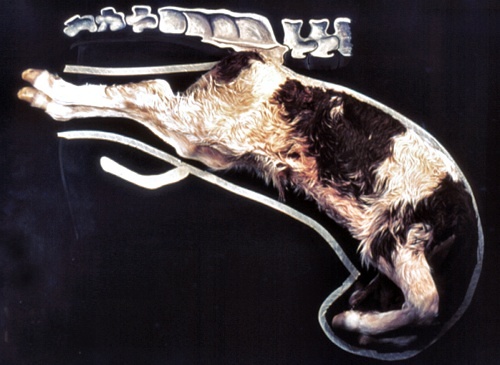
Dorso-Pubic Position.
In contrast with the equine fetus, it is highly unusual for the bovine fetus to be in a dorso-pubic position. In the cow the greater curvature of the uterus is dorsal. When the fetus does appear to be on its back, the clinician should rule out a torsion of the uterus.
Drost M (1976)
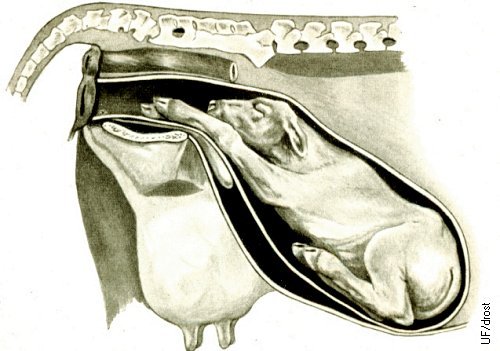
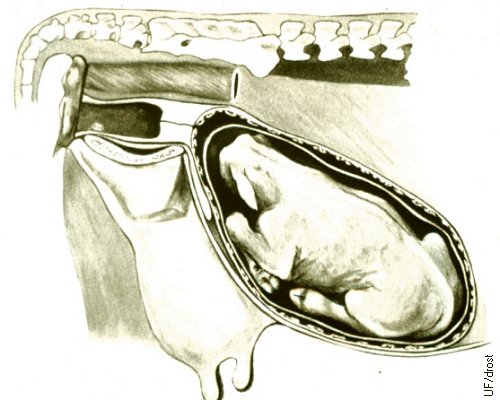
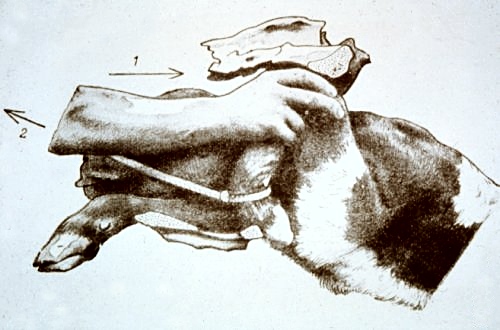
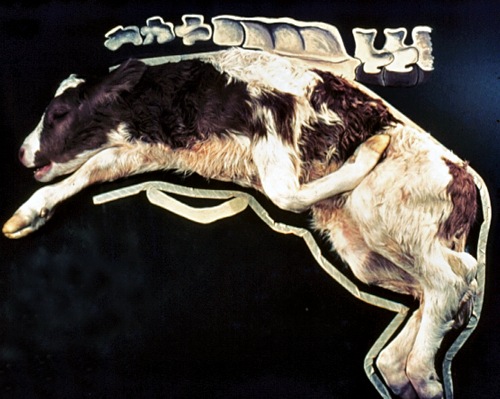
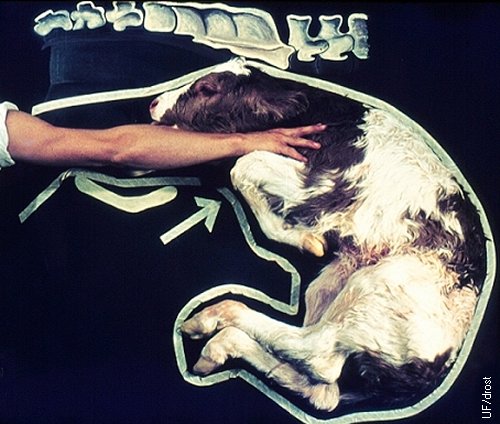
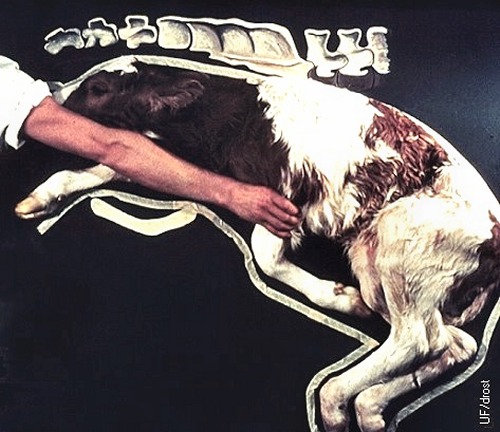
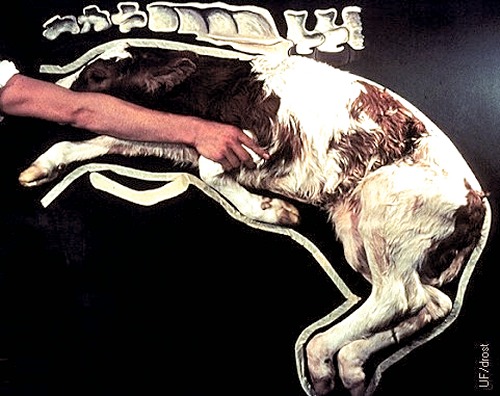
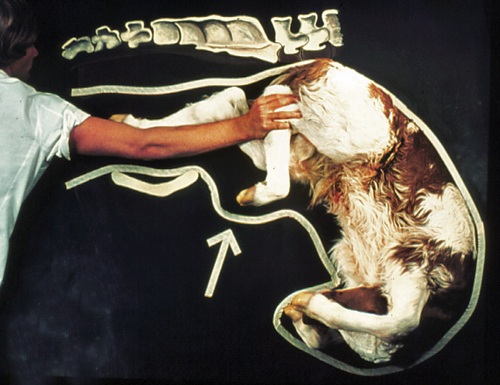
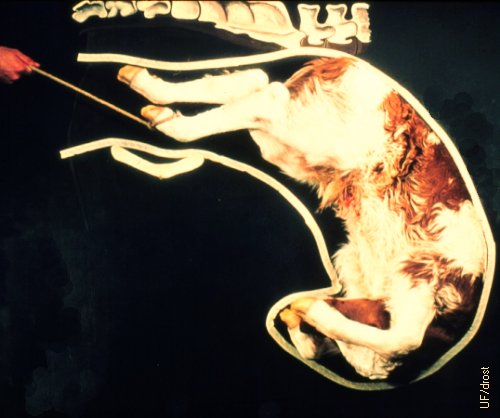
True Breech.
This calf is in posterior longitudinal presentation, dorso-sacral position, with both hind legs retained at the hips. In this position the calf does little to dilate the birth canal and the absence of fetal parts in the vagina leads to failure of the Ferguson reflex.
Drost M (1976)

Excessive Traction.
Forceful traction with mechanical aids is risky and may cause serious injuries to the calf and the dam. Guidelines outlined in the calving plan should be followed before extraction is started. This is no place and time for trial and error. Cleanliness and lubrication are the hallmarks of good obstetrics.
Drost M (1976)

Stretching the Vulva.
After it has been determined that there is enough room for the calf to be delivered per vaginam, it is helpful to stretch the lips of the vulva, especially in heifers. With the heifer standing, the forearms are inserted halfway to the elbows. Next, with the fingers folded, the arms are wedged apart in the direction from 11 o'clock to 5 o'clock and alternately from 7 o'clock to 1 o'clock, for 10 or more repetitions. After this the heifer is cast and the calf is extracted.
Haibel GK (1983)

Casting the Cow.
After it has been determined that there is enough room for the calf to be delivered per vaginam, the cow is cast in (preferably) right lateral recumbency. This 1) allows the hind legs of the dam to angle forward, which enlarges the operative diameter of the pelvis; 2) lets the heifer slightly spread her legs and stretch the cartilaginous symphysis pubis; 3) aid the calf in coming through the birth canal in a plane parallel to the ground, versus having to rise from the bottom of the abdomen - against the force of gravity - to enter the pelvic inlet; 4) virtually all cows go down during the second stage of parturition, hence it is better to cast them in a preselected location with sufficient room behind the cow to assist her.
Drost M (1983)

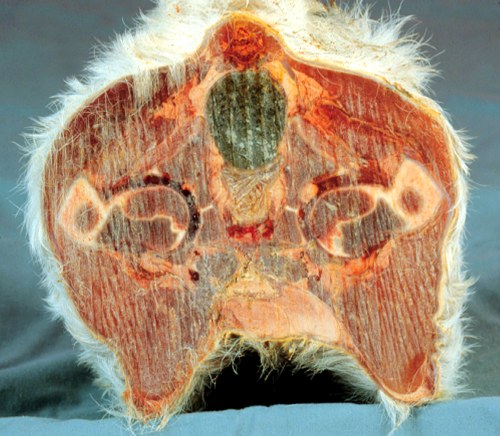
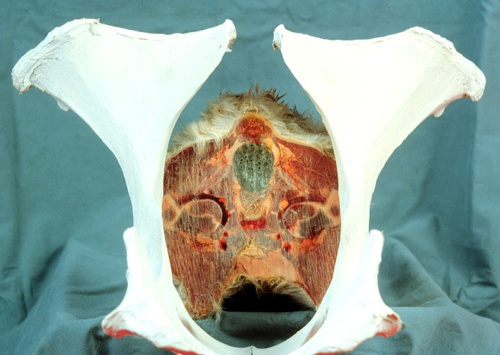
Maternal Pelvis.
The diameter of the bovine pelvis is oval whereby the vertical diameter is greater than the horizontal diameter. In addition the dorsal horizontal diameter is somewhat greater than the ventral one.
Drost M (1991)
Cross Section of the Fetus at the Hips.
The cross section of the fetus at the level of the hips, through the greater trochanters, is wider (horizontally) than it is tall (vertically). This is just opposite to that of the pelvis of the cow.
Drost M (1991)
Fetal Hips Entering the Pelvic Inlet.
The width of the hips of this large calf is wider than the that of the pelvic inlet. Note that the greater trochanters are hidden laterally behind the iliac shafts.
Drost M (1991)
Rotation of the Fetal Pelvis.
To prevent hiplock the fetus should be rotated as it enters the pelvic inlet, allowing the greater trochanters more space.
Drost M (1991)

Starting the Delivery.
The cow is cast, the assistants are in place, ready for the command of the obstetrician to pull in synchrony with the expulsive efforts of the cow.
Utrecht (1976)

When Head is Out: Stop.
As soon as the head is out, stop pulling. The assistants switch to pulling on the opposite leg and the obstetrician places one arm and hand all the way underneath the calf and inserts the other hand between the legs, and folds the fingers above the head, locking them with the fingers of the other hand. When the cow strains, he orders the assistants to pull while he pulls the head towards his / her knees thereby rotating the calf and the hips (as illustrated in the next image).
Utrecht (1976)

Start Rotation.
Rotation is started as soon as the head of the calf is out. The obstetrician places one arm all the way under the calf and inserts the other arm between the legs. The fingers are then folded and the head is pulled towards the knees when traction is applied in synchrony with the expulsive efforts of the cow.
Utrecht (1976)

Chest Out - Rotated 45 Degrees.
The calf has been rotated about 45 degrees. The hips are now past the iliac shafts of the cow. At this stage the hips are rotated back to a dorso-sacral presentation and the calf is pulled in a downward arch towards the udder of the cow.
Utrecht (1976)

Working the Vulvar Lips Over the Hips.
The vulvar lips frequently delay progress. The labia should be stretched over the greater trochanters of the calf with the flat of the hands.
Utrecht (1976)

Propping up the Calf for Ease of Respiration.
As soon as the calf has been delivered the immediately concern is that it is breathing. It is best to place the calf in sternal recumbency to allow both sides of the chest to expand.
Utrecht (1976)

Suspending the Newborn Calf.
While a common practice among lay people, suspending the calf by the hind legs is not recommended. In doing so the full weight of the viscera is on the diaphragm of the calf, and compresses the lungs. This makes it more difficult for the calf to breathe (expand its lungs) rather than easier. There is no fluid in the lungs of the newborn calf, they are consolidated (atelectic) prior to the first breath. There is a small amount of mucus in the trachea and the nostrils. The latter can be squeezed by stripping the nasal passages from the eyes towards the nostrils. Mucus seen running from the mouth and nose of the suspended calf is actually amniotic fluid coming from the stomach. [Meconium staining denotes intrauterine hypoxia].
Drost M (1966)
Colostrum.
It is important that the newborn calf gets about 3 to 4 liters of good quality colostrum within the first two hours after calving.
Drost M (1983)


Obstetrical Phantom - Posterior View.
Mechanical frame of the birth canal as a teaching aid for determining the presentation, position, and posture of the calf. Stillborn calves or large, near term fetuses can be used. The phantom can also be used for learning how to perform a fetotomy. Dimensions: legs 103 cm long; horizontal bar at the bottom 71 cm; top ends of the legs 18 cm apart.
Drost M (2009)

Obstetrical Phantom - Vestibule.
Posterior diameter of the birth canal. Internal diameter of the circle: 30 cm.
Drost M (2009)

Obstetrical Phantom - Lateral View.
Left lateral view of the obstetrical phantom. The pelvic floor is horizontal. The slope towards the abdominal cavity is approximately 45 degrees. Dimensions: bent legs 113 cm + 22 cm for the short vertical end.
Drost M (2009)

Obstetrical Phantom - Pelvic Area.
Right lateral view of the pelvic area. The pelvic floor is horizontal. The slope into the abdominal cavity is approximately 45 degrees. The oval arch on the right represents the pelvic inlet.
Drost M (2009)

Obstetrical Phantom - Anterior View.
The oval pelvic inlet is at the top (vertical diameter 30 cm, horizontal diameter 24 cm). The sloping abdominal floor is made out of sheet metal. The upper edges curve inwards (width of the curved area is 10 cm at the top). Dimensions: width of the sheet metal at the bottom is 68 cm; horizontal bar at the bottom is 78 cm; distance between the edge of the sheet metal and the horizontal bar is 20 cm.
Drost M (2009)

Obstetrical Phantom - Anterior View.
The oval pelvic inlet is at the top. The uterus is a large bag which is completely unzipped in this image.
Drost M (2009)

Obstetrical Phantom - Anterior View.
The oval pelvic inlet is at the top. The uterus is a large bag which can be opened and closed with a full length zipper.
Drost M (2009)