
Perineal Conformation.
Normal perineal conformation. The alignment of the anus and vulvar lips is approximately vertical.
Asbury AC (1986)

Normal Perineal Conformation.
Close-up of normal perineal conformation in a mare. Vertical orientation.
Asbury AC (1986)

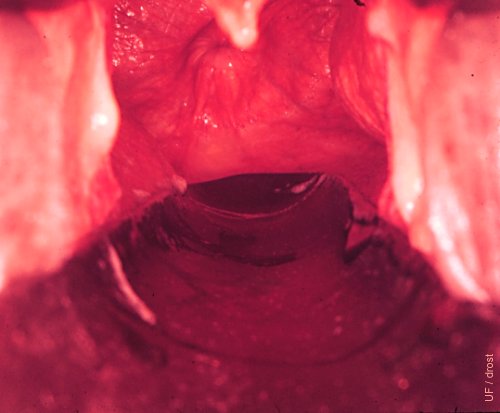
Persistent Hymen.
Developmental defect whereby the caudal end of the paramesonephric duct (Mullerian duct) fails to join the invagination of the vestibule.
Roberts SJ (1972)

Pelvic Floor.
The finger indicates the location of the level of the pelvic floor.
Asbury AC (1986)

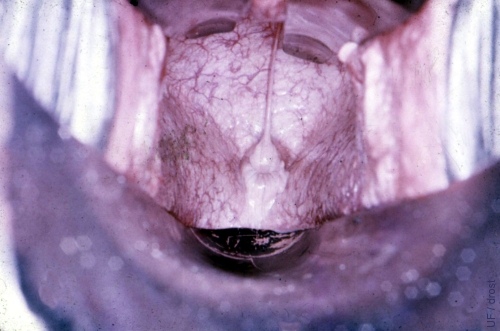
Vulvovaginal Sphincter.
The vulvovaginal sphincter is intact and normal.
Asbury AC (1986)

Clean-up for Vaginoscopy.
Proper clean-up prior to insertion of the vaginoscope is essential. The anus in this mare is pulled slightly forward.
Asbury AC (1986)

Insertion of the Tube Speculum.
After wrapping the tail and cleaning the perineum and vulva, one labium is pulled slightly to the side and the speculum is gently introduced.
Asbury AC (1986)

Tube Speculum Inserted.
The glass tube speculum has been fully inserted. Air will be aspirated and the vagina will balloon allowing detailed inspection of its wall and of the cervix. A bright light source is used.
Asbury AC (1986)

Caslick Speculum.
After washing the mare the Caslick vaginal speculum is ready for insertion. Prior to insertion the split dorsal blades and wider ventral blade are rotated a quarter of a turn. After insertion the blades are rotated back 90 degrees. The divided upper blades can opened up laterally by turning the large wing nut.
Asbury AC (1986)

Caslick Speculum in Place.
The Caslick speculum is fully inserted and the blades have been expanded. The bright speculum light is positioned to permit viewing of the cervix and the vagina, as well as possible secretions.
Asbury AC (1986)

Vaginoscopy.
The cervix and vagina are examined with a sterile cylindrical glass speculum [length 45 cm, diameter 4 cm] and a speculum light.
Asbury AC (1986)
Vaginitis.
This mare had an endometritis as well as a vaginitis. Note the pronounced hyperemia of the vaginal mucosa. There was no gross vaginal discharge. Vaginoscopic view.
Hughes JP (1961)
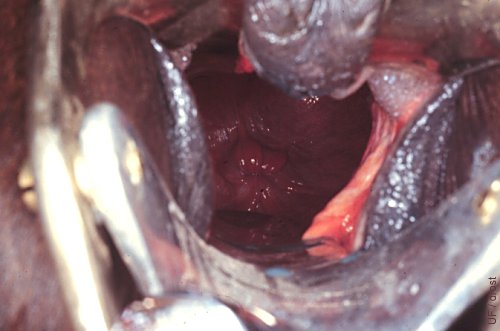
View of an Anestrous Cervix.
Direct view of the external cervical os with the aid of a Caslick speculum. The darker lower portion of the image is the large ventral blade of the speculum.
Asbury AC (1986)
View of an Estrous Cervix.
The cervix is edematous and relaxed during estrus. Vaginoscopic view.
Grimmett JB (1981)

Checking for Pneumovagina.
Technique for evaluation of pneumovagina. While slightly parting the labia a tube speculum is slowly inserted to observe whether the vulvovaginal sphincter dilates when air enters the vestibule.
Asbury AC (1986)

Abnormal Perineal Confirmation.
Close-up of abnormal perineal confirmation. This mare is a candidate for pneumovagina. The anus is sunken in and the vulvar cleft is slanted forward.
Asbury AC (1986)

Sunken-in Anus.
In this older mare the anus is sunken in and appears to have been pulled forward. The dorsal portion of the vulva lies horizontally. When the tone of the labia is also poor, fecal juice may enter the vagina and cause contamination. Such mares may also be windsuckers.
Asbury AC (1986)
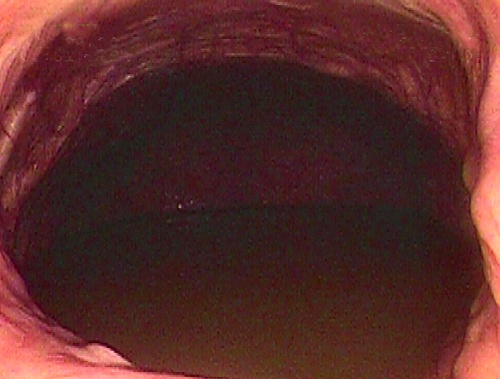
Vaginal Endoscopy.
An endoscope was inserted into the cranial vagina of a mare. The vagina sloped cranio-ventrally, causing severe pooling of urine, extending into the uterus. The cervix is completely submerged.
King AC (2008)
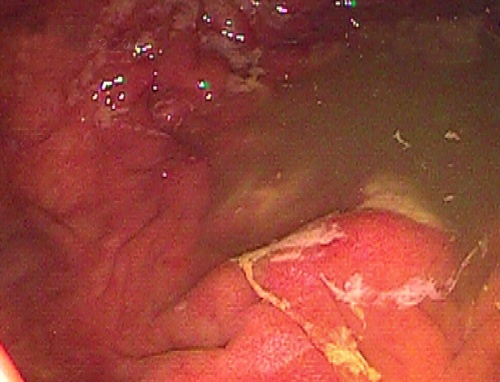
Intrauterine Urine Pooling.
The endoscope was inserted through the cervix into the uterine body of the mare. Chronic, severe urine pooling has caused irritation of the uterine lining; fibrin strands can be seen adhered to the luminal surface of the endometrium.
King AC (2008)

Urine Pooling in the Uterus.
The endoscope was passed via the cervix into the uterine body. Here we can see the bifurcation of the uterine horns. Urine can be seen pooling in both uterine horns.
King AC (2008)

Perianal Abscess.
A perianal abscess is located at the 4 o'clock position in relationship to the anal sphincter. The ventral portion of the vulvar lips is slightly parted. These lesions are likely sequelae to a traumatic delivery. This mare is likely to develop a pneumovagina.
Asbury AC (1986)
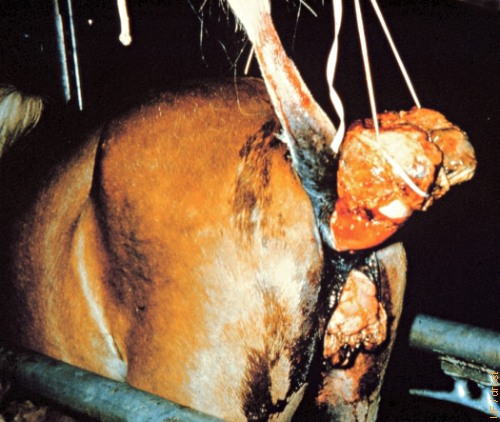
Prolapsed Vagina and Rectum.
Massive prolapsed rectum and vagina. The mare recovered following surgical excision of the indurated tissues.
Roberts SJ (1972)