
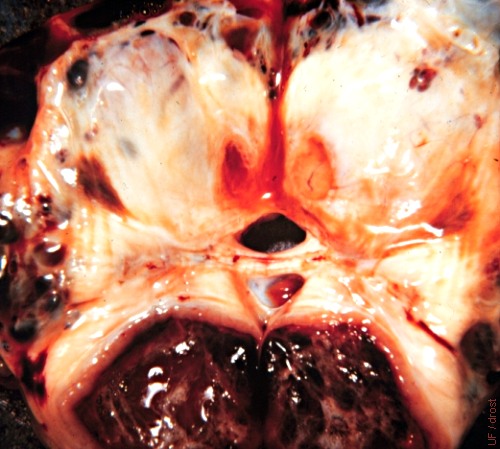
Ovulation Fossa.
Upon ovulation, the equine follicle releases its ovum into the ovulation fossa. The opening can be seen below and to the right of the reddish tissue.
Roberts SJ (1972)
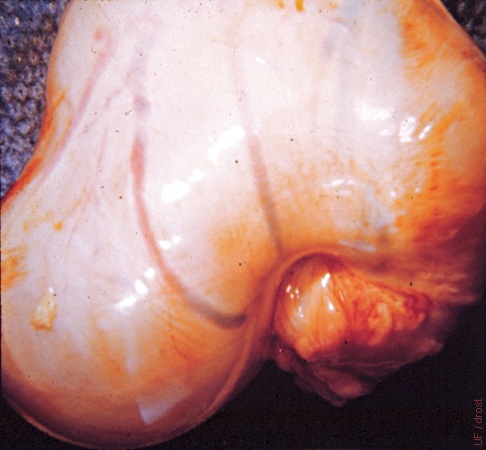
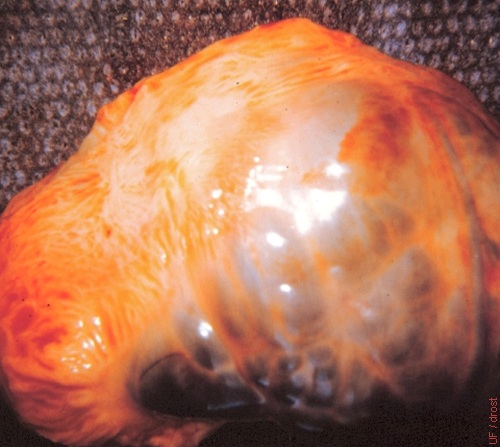
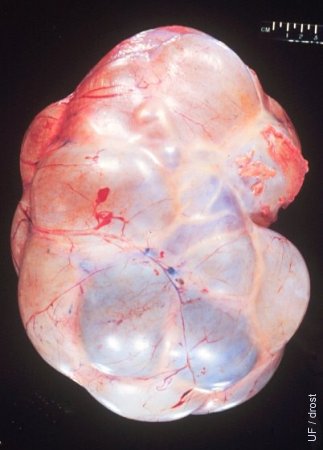
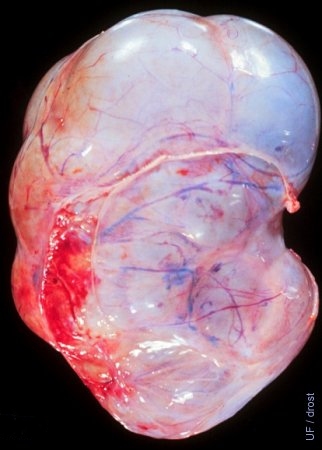
Ovulatory Follicle.
Large ovulatory follicle of a mare in estrus.
Roberts SJ (1972)
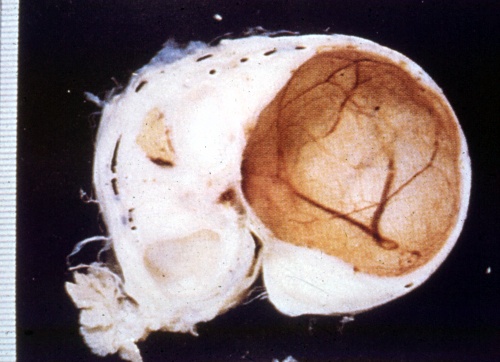
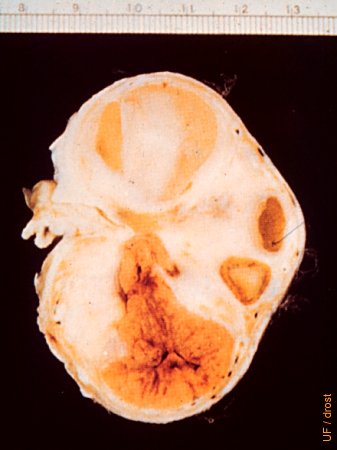
Graafian Follicle.
Cross section of the ovary of a mare showing an ovulatory follicle, sometimes called a Graafian follicle.
Roberts SJ (1972)
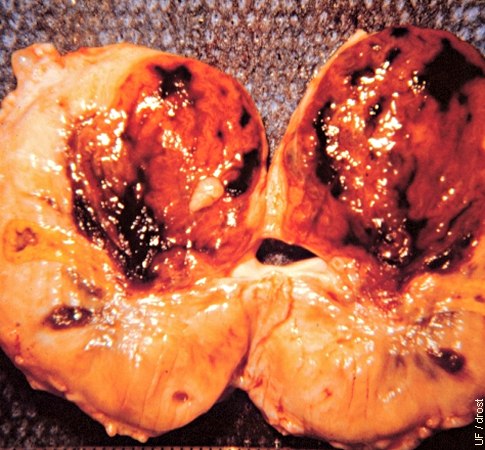
Fresh Ovulation.
Cross-section of the ovary. After ovulation the follicular cavity is filled with a fresh dark blood clot.
Roberts SJ (1972)

Recent Ovulation < 6 hours.
Ovulation occurred approximately six hours earlier. The follicular cavity is filled with a large blood clot.
Roberts SJ (1972)
Recent Ovulation < 24 hours.
Ovulation via the ovulation fossa occurred less than 24 hours ago. Blood and early luteinization are visible on cross-section of the ovary.
Roberts SJ (1972)
Corpus Luteum.
The corpus luteum is shown on cross section of the ovary. The follicle releases the ovum via the ovulation fossa, hence there is no ovulation papilla (crown) on the surface of the ovary as there is in the cow.
Roberts SJ (1972)

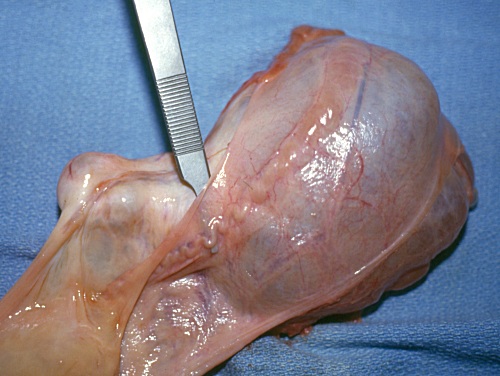
Large Fimbrial Cyst.
Several ovarian follicles and a fairly large fimbrial cyst. The latter may be confusing on an ultrasonogram.
Roberts SJ (1972)

Fimbrial Cysts.
There is no ovarian activity. There are several several small fimbrial cysts along the edge of the ovarian bursa. There is also a fibrin tag at the ovulation fossa.
Roberts SJ (1972)
Ovarian Varicose Veins.
Obstruction and enlargement of the veins of the ovary leads to development of varicose veins. Occasionally thrombi occur.
Roberts SJ (1972)

Venous Varicoses.
Cross-section of an ovary showing multiple varicose veins.
Roberts SJ (1972)

Ovaries with Pyometra.
Ovaries from a mare with pyometra, showing varied follicular activity.
Roberts SJ (1972)
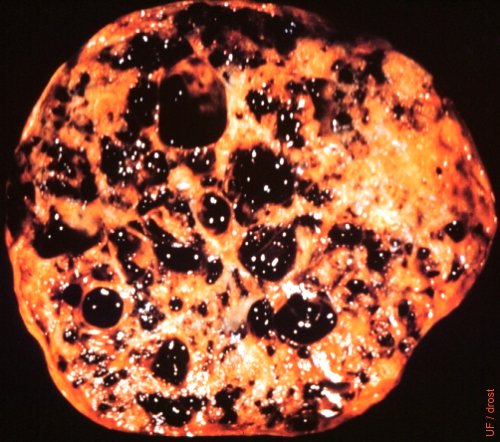
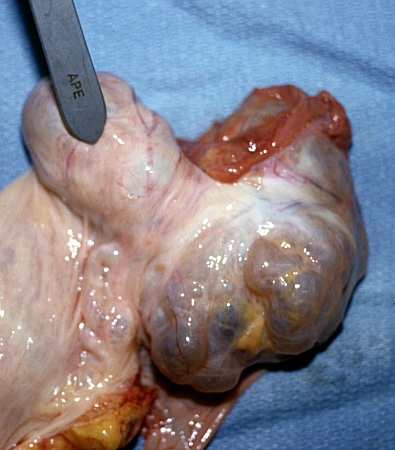
Granulosa Cell Tumor.
Cross-section of a polycystic granulosa cell tumor. Many are hormonally active, producing estrogen. Most common ovarian tumor in the mare.
Roberts SJ (1972)

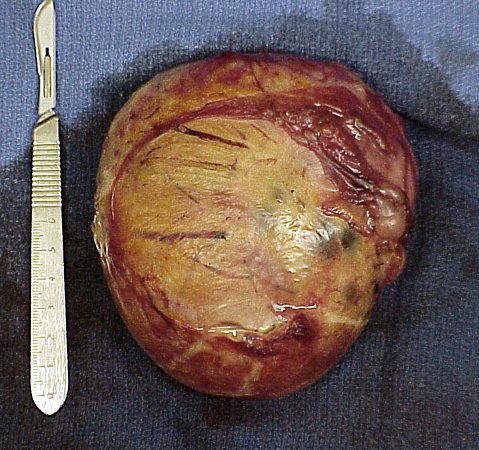
GCT Surgically Removed.
This granulosa cell tumor was surgically removed via a flank laparotomy. The ovary was large and firm on palpation.
King AC (2008)

GCT Cross Section.
Cross section of a granulosa cell tumor following surgical removal, showing the multilocular, cystic structures typical of this type of tumor. In addition to secreting inhibin, these tumors frequently secrete testosterone causing the mare to exhibit stallion-like behavior.
King AC (2008)

Granulosa Cell Tumor - Cross Section.
Cross section of a granulosa cell tumor following surgical removal showing the multilocular, cystic structures typical of this type of tumor. In addition to secreting inhibin these tumors frequently secrete testosterone causing the mare to exhibit stallion-like behavior.
Shipley C (2006)

Serous Cystadenoma.
This is a rare polycystic tumor. These tumors appear to be endocrinologically inactive.
McEntee K (1972)
Cystadenoma.
Rare ovarian tumor that is not accompanied by aberrant reproductive behavior.
McEntee K (1972)
Cystadenoma.
Rare ovarian tumor that is not accompanied by aberrant reproductive behavior.
McEntee K (1972)

Parovarian Cysts.
These are large bilateral parovarian cysts. The ovaries are located near the tip of the horns.
Shipley C (2006)

Parovarian Cyst Close Up.
The small inactive ovary is in the upper right. There is a normal Fallopian tube which is slightly distended near the end as it crosses the parovarian cyst.
Shipley C (2006)

Parovarian Cyst.
There is a small inactive ovary near the tip of the right horn. The Fallopian tube is normal. There is a cyst inside the ovarian bursa.
Shipley C (2006)
Parovarian Cyst.
The ovary per se is pushed aside. The Fallopian tube is normal.
Shipley C (2006)
Parovarian Cyst.
The small inactive ovary is on the left. The Fallopian tube is normal and stretched out over the large parovarian cyst.
Shipley C (2006)
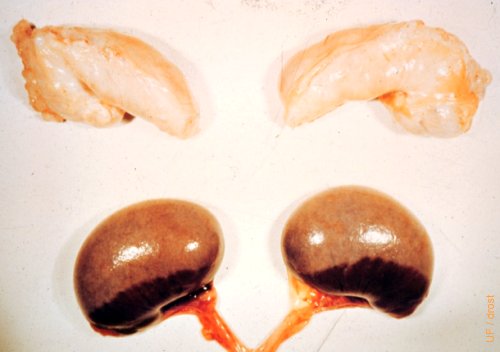
Fetal Ovaries.
Comparison between the fetal ovaries from a 5-month old fetal filly with those of a normal anestrous adult mare at the top. The tan colored portion is the medulla, the dark brown area the cortex near the hilus.
Roberts SJ (1972)
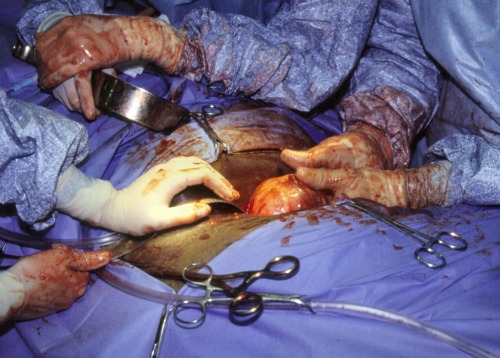
Ovarian Tumor Exposed.
Surgical removal of a granulosa cell tumor.
Pozor MA (2009)
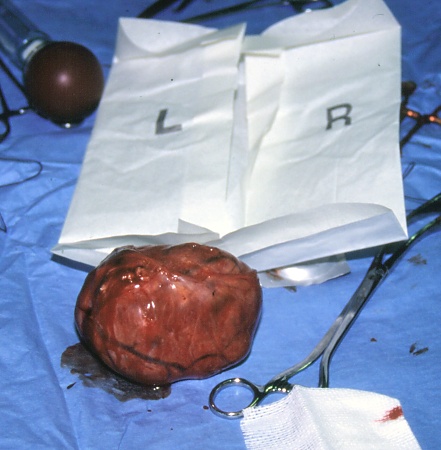
Granulosa Cell Tumor.
Granulosa cell tumor surgically removed from the mare.
Pozor MA (2009)

Colpotomy: Chain Ecraseur.
The snare of this ecraseur is a sharp flexible chain which is used to crush and cut through the pedicle of a tumor, or an ovary, to minimize hemorrhage.
Hopper RM (2010)

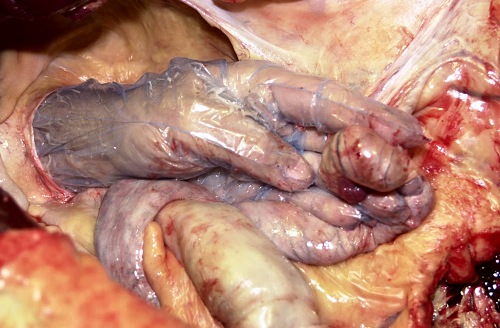
Colpotomy: Stab Incision.
One gloved finger is inserted through the stab incision in the fornix, and it enters the peritoneal cavity of this cadaver specimen. Notice the flaccid horns of the uterus. For a live mare she is sedated and given epidural anesthesia. It is imparative to induce pneumovagina to stretch the vaginal wall. A 2 to 3 cm incision is made in the fornix at a 10:00 or 2:00 o'clock position [depending on whether one uses the left or right hand respectively].
Hopper RM (2010)
Colpotomy: Insertion of a Hand.
After insertion of one finger, two fingers then three fingers, and ultimately the entire hand, they are forced through the incision to enlarge it by blunt dissection. Now the ovary can be palpated directly.
Hopper RM (2010)
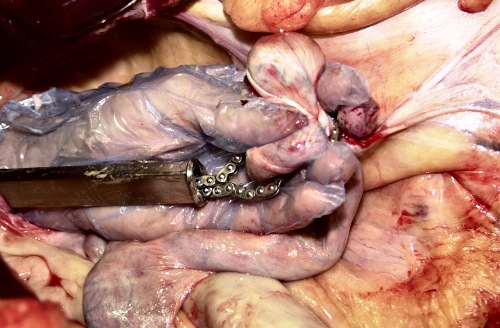
Colpotomy: Placement of the Ecraseur.
The loop of the chain of the ecraseur is placed around the pedicle of the ovary after insertion of the ecraseur through the initial stab incision. Care is taken to avoid including part of the uterus or viscera.
Hopper RM (2010)
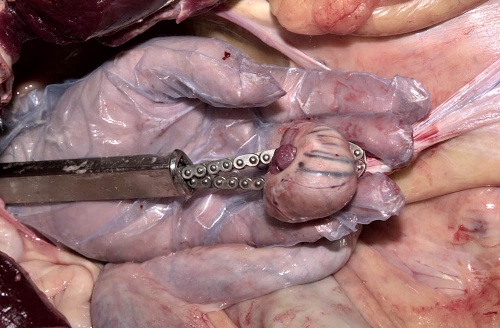
Colpotomy: Chain in Place.
The chain of the ecraseur has been placed around the pedicle and directly adjacent to the ovary.
Hopper RM (2010)
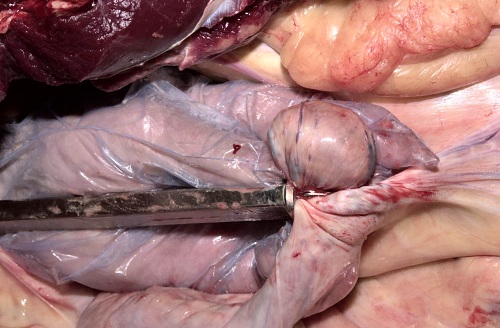
Colpotomy: Chain Pulled Tight.
The chain of the ecraseur has been pulled tight around the pedicle. The ovary is ready to be severed.
Hopper RM (2010)
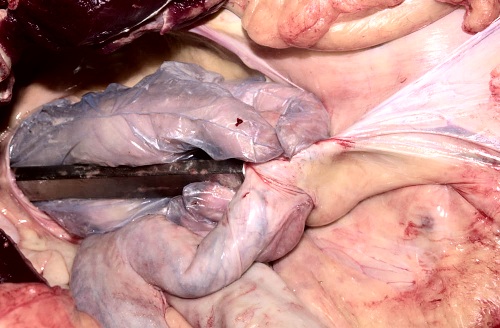
Colpotomy: Ovary Cupped in Hand.
The ovary has been cupped in the hand to prevent it from dropping into the peritoneal cavity upon severing with the chain of the ecraseur.
Hopper RM (2010)

Colpotomy: Severed Ovary.
Ovary severed with the ecraseur is ready for retrieval via the vagina. The amount of hemorrhage is minimal with the procedure in a live mare. The process can be repeated for the contralateral ovary via the same incision in the fornix.
Hopper RM (2010)