The Visual Guide to
Equine Reproduction
- Parturition
- Presentation
- Injuries to the Foal
- Cesarean Section
- Fetotomy
- Twinning
- Prolapsed Uterus
- Prolapsed Rectum
Obstetrics: Parturition

Waxing of the Teats.
Colostrum starting to drip from the teat in response to oxytocin pulses as early as 24 hours prior to parturition.
Utrecht (1976)

Foaling Sequence 1.
Stage 1 of parturition, the stage of preparation is characterized by uterine and some abdominal contractions. The mare gets up and down and strains. During this stage the foal rotates from a dorso-pubic position into a dorso-sacral position and the cervix begins to dilate.
Asbury AC (1977)

Foaling Sequence 2.
Stage 2 of parturition is heralded by the appearance of membranes at the vulva. Straining continues and intensifies. Stage 2 is the stage of expulsion of the fetus.
Asbury AC (1977)

Foaling Sequence 3.
Stage 2 of parturition continues with the appearance of fetal extremities.
Asbury AC (1977)

Foaling Sequence 4.
Stage 2. More fetal parts appear, including the muzzle when the foal is in anterior presentation.
Asbury AC (1977)

Foaling Sequence 5.
Late Stage 2, the head of the fetus has been delivered. An assistant may tear the membranes away from the nostrils of the foal, allowing it to breathe.
Asbury AC (1977)

Foaling Sequence 6.
Stage 2 nearly completed. Membranes should now be removed from the face of the fetus to allow it to breathe. The umbilical cord remains intact until the mare gets up. This permits the so-called placental transfusion to take place. The cord should not be cut nor ligated.
Asbury AC (1977)

Foaling Sequence 7.
Stage 2 complete. The foal has been delivered. The long umbilical cord frequently remains intact until either the foal or the mare moves away.
Asbury AC (1977)


Foaling Sequence 9.
The mare is up to examine and lick the foal. The latter stimulates respiration.
Asbury AC (1977)

Foaling Sequence 10.
The foal is up. The fetal membranes are hanging from the vulva. They are usually spontaneously delivered within 6 to 8 hours. If they are not expelled by 12 hours the placenta is considered retained and intervention is needed.
Asbury AC (1977)

Beginning of Stage 2.
The burst of allantoic fluid heralds the onset of Stage 2 of parturition, the stage of expulsion of the fetus. Defecation frequently accompanies straining and soils the obstetrical area.
Drost M (1976)

Amnion Showing.
After rupture of the chorioallantois there is usually a pause in labor. The next thing to show is the amnion, a greyish blue membrane.
Drost M (1976)

Limb Showing.
Is it a front leg or a hind leg? Is the foal presented anteriorly (head first) or posteriorly (tail first)?
Drost M (1976)

Head Out.
As the head emerges the umbilical cord is still intact. The amnion may have to be cleared away from the nostrils.
Drost M (1976)

Rupture of the Chorioallantois.
Rupture of the chorioallantois occurs at the beginning of Stage 2 of parturition. The mare has been cleaned up and prepared for delivery.
Drost M (1976)

Delivery of the Placenta.
Stage 3, delivery of the fetal membranes.
Drost M (1976)
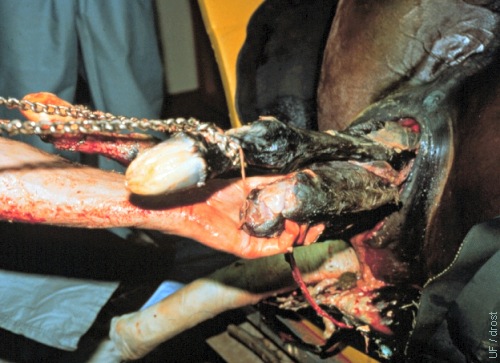
Dystocia.
The mare is in dorsal recumbency under general anesthesia. One final attempt is made to extract the fetus, before resorting to a cesarean section. The legs are coated with Vaseline.
Drost M (1980)

Dry Fetus.
The fetus is dry which suggests that the mare had been in labor for a considerable time.
Drost M (1980)

Mare in Sling.
Pregnant mare that foundered was intermittently suspended in a sling to await a terminal cesarean section.
Pozor MA (2009)

Lateral Recumbency.
Foundered pregnant mare in lateral recumbency, prepared for and awaiting a terminal cesarean section. White circles are electrodes for monitoring fetal viability.
Pozor MA (2009)

Retained Placenta.
The placenta (actually the fetal membranes) are normally spontaneously delivered within 6 to 8 hours. They are considered retained when not expelled by 12 hours after delivery of the foal.
Asbury AC (1977)
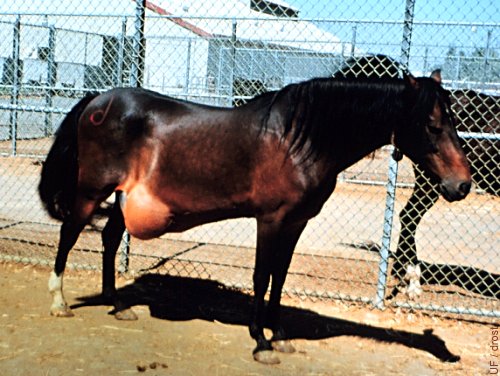
Ventral Abdominal Hernia.
Ventral abdominal hernias may present a problem in the advanced pregnant mare as a result of increasing abdominal pressure.
Grimmett JB (1981)

Abdominal Edema.
Physiological abdominal edema is common in the mare and may indicate a possible weakness of the abdominal floor.
Utrecht (1975)

Excessive Edema.
Excessive edema may lead to circulatory impairment and sloughing of the skin, requiring wound care.
Utrecht (1975)

Circulation Disrupted.
Pressure necrosis and sloughing of the skin due to excessive edema.
Utrecht (1975)

Transudate.
Impaired circulation led to fluid accumulation and sloughing of the skin with drainage of a transudate.
Utrecht (1975)